
A Tree Feller Dies When Struck By a Tree Limb While Felling a Fire-Damaged Tree
-
Fatality Assessment and Control Evaluation (FACE) Program Reports
The National Institute for Occupational Safety and Health’s (NIOSH) Fatality Assessment and Control Evaluation (FACE) Program and State FACE Programs study fatal workplace injuries and prepare reports with recommendations to prevent similar injuries. The following are links to all of the items in this collection:
Documents
- Kentucky FACE Report: Commercial Roofer Falls 30 Feet Through a Skylight While Installing Roof Insulation
- Fatal Occupational Injuries in Massachusetts 2008-2013
- Fatality Assessment & Control Evaluation (FACE) Program
- Washington FACE Report: Glazier Foreman Falls From Stepladder
- Preventing Construction Falls Toolkit
- Hazard Alert: Pedestrian Workers Killed by Forklifts
- Keep Employees in Motor Vehicles Safe
- New York FACE Brochure
- Washington FACE Report: Construction Laborer Falls When Ladder Breaks
- Washington FACE Report: Pipelayer Dies when Trench Wall Collapses
- Washington FACE Report: Carpenter Falls 60 Feet from Bridge Concrete Form
- Washington FACE Report: Foreman and Laborer Fall when Aerial Lift Struck by Vehicle
- Washington FACE Report: Framer Falls 18 Feet while Sheathing Roof
- New York FACE Report: Mechanic Electrocuted when a Mobile Light Tower Contacted Powerline
- New York FACE Report: Two Construction Workers Fatally Crushed when Cement Formwork Collapsed
- Kentucky FACE Report: Construction Laborer Killed in Trench Collapse while Taking Grade Measurements
- California FACE Report: A Heating, Ventilaton and Air Conditioning (HVAC) Contractor Dies when He Falls through a Skylight
- Massachusetts FACE Report: Carpenter Fatally Injured after Falling from an Extension Ladder
- Massachusetts FACE Report: Laborer Fatally Injured after Falling from a Home under Construction
- Oregon FACE Report: Worker Falls When Ladder Slips
- Michigan FACE Information Sheet: Look for Mobile Equipment Blind Spots
- Oregon FACE Report: Collapsed roof trusses kill carpenter foreman
- Washington FACE Report: Roofer Falls 19 Feet from Roof
- Hazard Alert: Plan. Provide. Train. Prevent Fall Injuries & Deaths
- Kentucky FACE Report: 19-Year-Old Construction Laborer Crushed in Trench Collapse While Laying Sewage Pipe
- Kentucky FACE Report: Construction Flagger Struck and Killed in Two-Lane Highway Work Zone
- Kentucky FACE Report:Temporary Electrician Helper Steps into Unguarded Elevator Shaft and Dies
- Fatality Narrative: Roofing Contractor Falls 25 Feet From Church Roof
- Kentucky FACE Report: Construction Siding Subcontractor Installer Killed when Oversized Scaffolding Platform Destabilized and Telescopic Forklift Overturned
- NIOSH FACE Report - Maintenance Worker Struck by Forklift Carriage—Tennessee
- Kentucky Hazard Alert: Roofing and Construction Workers Killed Due to High Winds
- Poster: Secure it to move it!
- Oregon FACE Report: Crane Operator Killed By Falling Steel Beam
- New Jersey FACE Report: Mechanic Dies After Being Crushed Under Electrical Cabinet
- New Jersey FACE Report: Plant Manager Crushed to Death Under Fallen Pile of Steel Beams
- NIOSH FACE Report: Hispanic worker falls from residential roof
- Oregon FACE Report: Construction worker died after falling 20-25 feet from a pump-jack scaffold
- FACE Fact Sheet: Prevent Construction Falls from Roofs, Ladders, and Scaffolds
- Construction Fatality Narrative: Roofer Falls 18 Feet from Wet House Roof
- Construction Worker Killed when Trench Collapsed, Oregon
- A Tree Trimmer is Electrocuted While Trimming a Palm Tree
- A Tree Feller Dies When Struck By a Tree Limb While Felling a Fire-Damaged Tree
- Concrete Finisher Electrocuted When Bull Float Contacted an Energized Power Line
- Warehouse Worker Crushed by Forks of Laser Guided Vehicle
Summary Statement
A 21-year-old male tree feller, working from a bucket truck as part of a small tree-felling crew, died when struck by a large tree limb he had just cut. The 80 to 90-foot, fire-damaged oak tree was located below a county road that ran along the steep bank of a creek ravine. The crew had been directed not to fell the tree into the ravine because of environmental and cultural concerns. The crew had been directed to take the tree down in small sections. However, after the supervisor left, the victim decided that they should attempt to bring most of the tree down in two large sections. The crew used a rigging line, pulled by a mini-excavator, to attempt to direct the cut sections to fall uphill towards the road. Neither section fell in the direction intended; the second section fell uphill against the bucket truck, fatally crushing the victim.
The California Fatality Assessment and Control Evaluation Program (CA/FACE) concluded that organizations involved in tree-felling operations should take the following steps to prevent similar incidents:
- Tree-felling contractors should ensure that each crew includes, and is led by, a person with substantial experience in tree felling.
- Tree-felling contractors should ensure that all supervisors are certified in tree-felling safety by an organization such as the Tree Care Industry Association (TCIA) or the International Society of Arboriculture (ISA). In addition, government agencies, utilities, and other project customers should include bid language requiring that all supervisors be certified in tree-felling safety by one of these organizations.
- Tree-felling crews should always be able to readily communicate with their supervisor and medical emergency services. If cell phone reception is not reliable, the employer should issue the crew a satellite phone.
April 2019
Introduction
On April 6, 2017, at approximately 11 am, a 21-year-old male tree feller, working from a bucket truck as part of a crew, died when struck by a large tree limb. The CA/FACE program learned of the fatality from the California Department of Industrial Relations on April 12, 2017. The CA/FACE investigator visited the worksite and interviewed Cal/OSHA enforcement staff on January 18, and interviewed the site environmental monitor on February 23, 2018. Numerous unsuccessful attempts were made to interview co-workers or the contractor. In addition, a trade association representative and a tree felling contractor were consulted for assistance with technical interpretation and assessment.
Project and Employers
After a fire burned 70,000 acres in the California Sierra foothills in the late summer of 2015, the county received Federal Emergency Management Agency (FEMA) funding to remove approximately 8,000 roadside ‘hazard trees’— which were burned and in danger of falling onto roads. The work began in late 2016.
Initially the general contractor (general) selected three local contractors to do the on-the- ground work. However, rains slowed the release of the work, and only one local subcontractor (subcontractor) was eventually hired, as this company reportedly appeared able to keep up with the work. This subcontractor was a local, husband-and-wife-owned transportation and logging company, in business since 2005. The victim started working for this company in November 2016. In January 2017, this same couple formed a second company focused on tree- felling operations. The victim then moved over to work for this second company. At the time of the incident, the company had 25 employees working in six crews on this county tree removal project.
The county also hired an independent consulting company to oversee the expenditure of federal funds and to ensure that all regulations were followed. This company subcontracted to specialists to provide biological, archeological, and cultural monitors as on-site monitors to ensure the safeguarding of environmental and cultural resources.
Written Safety Programs, Worker Training, Experience, and Knowledge
At the time of his death, the victim had approximately 3½ years’ experience in the tree industry with three companies: for a local tree felling company as a sawyer/groundsman, for a communications company working as a communications lineman, and for a heavy civil construction firm conducting roadside hazard tree removal. The victim’s father estimated that, prior to being hired by the subcontractor, his son had four months of part-time experience operating a bucket truck.
Prior to this job, the victim received training on basic safety topics, grinding and chipping operations, chain saw safety, and logging. He did not, however, receive training on the following topics: technical tree felling and cutting techniques (safe rigging application and set- up), rigging (chokers, cables, shackles, mechanical advantage systems, etc.), and knot and hitches (groundsman, saw man, technical tree fellers, and climbers). Between initial hiring in November and assignment to the county hazard tree removal project at the end of January, the victim worked primarily as a groundsman setting ropes, rigging, and dragging branches. He was observed by the general’s supervisor and reportedly demonstrated good, precise use of the chain saw. His crew reportedly completed multiple technical tree fellings.
After moving to the county hazard tree removal project, the victim was again observed while climbing and was deemed to have the skills needed for taking down trees that do not present particular difficulties; he reportedly demonstrated good judgment and cautious decision- making. At the end of February, the victim began felling trees while operating a rental bucket truck (Altec 55-ft. forestry truck), and was assessed by management as being safe and competent. By the end of March, the crews were reconfigured and the victim was reassigned to a specific bucket truck crew. Since he was ‘in the tree,’ he was given the power to make crew decisions. He was reportedly observed by management a number of times and each time demonstrated “extreme caution and good judgment.” This reconfigured crew was young, the oldest being 25 years old.
During the project there were weekly mandatory tailgate safety meetings put on by the general. In addition, the subcontractor held daily safety and planning meetings for all employees. The general had an extensive written safety program.
Incident Scene
There were a number of ‘hazard trees’ along the road, which ran along the steep bank of the creek ravine. These hazard trees had been designated as such by the county arborist, because they were thought to be damaged and in danger of falling onto the road. Felling these trees was made more difficult because the subcontractor had been instructed not to fell trees into the ravine because of environmental and cultural concerns. Crews working in the ravine were observed by biological and cultural monitors, whose job it was to ensure that the crews adhered to this rule.
A number of these ravine hazard trees (including the oak tree) were considered to be particularly problematic. At one point the subcontractor considered bringing in a crane to remove these trees, but realized that there was not sufficient room for this equipment on the narrow road. Two additional issues complicated the proposed task of felling this particular oak tree. In addition to having sustained some fire damage, it had a large, pre-existing cavity at the base of the main trunk. This meant that the oak was possibly structurally unsound, and sending a climber up the tree to piece it down was ruled out as unsafe. For most of its 80 to 90-foot length, the tree leaned away from the road and down towards the bottom of the ravine. This limited the ability of the 55-ft. bucket truck to reach the upper portions of the tree from the road.
For two days prior to the fatal incident, the victim’s crew was climbing and felling trees down the road from the incident site. Meanwhile, the subcontractor had brought in a highly skilled crew from another project to use the bucket truck to piece down the ‘technical’ trees (those that required a high level of skill) along the ravine road. Whether the oak should have been included in this crew’s work is not clear. The general reported that, when the highly skilled crew left the ravine, the remaining trees, including the oak, were considered straightforward work.
A week prior to the incident, the crew’s immediate supervisor was removed from the job because of an altercation with one of the monitors. The owner of the subcontractor and the regional manager of the general took over crew supervision in the interim. On the day of the fatal incident, the owner of the subcontractor was collecting supplies in a nearby city, and the contractor’s regional manager was supervising the crews.
Investigation
On the morning of the incident, after the daily safety and planning meeting, the victim and his crew assembled at the site of the oak at approximately 7:30 am. The victim met with the general’s regional manager and the crew supervisor – no other crewmembers attended the job briefing. The general’s regional manager estimated the oak to be 80 feet tall with a maximum trunk diameter of 41 inches. The base of the tree was ten feet below the road. About 30 feet up, the trunk split into two large vertical spars which were each 16 to 18 inches in diameter. These two spars rose an additional 20 to 30 feet before spreading out into the canopy of the tree. The regional manager reported afterwards that they discussed piecing the tree down. He reported pointing out a dominant crotch in the tree approximately 50 feet above the road. He judged that this crotch was accessible using the bucket truck. From this crotch, the entire canopy of the tree was to be ‘pieced down’ using rigging and a tag line to pull the pieces down towards the road. After that, the spars and the trunk would also be pieced down by sequentially cutting off short sections from the top. The general regional manager later reported that the victim agreed to this plan, and pointed out the crotch which would be used for the initial work on the crown. The regional manager and the crew supervisor left immediately after the briefing, at about 7:45 am, to tour the rest of the project.
The evidence documented afterwards at the site indicates that the crew was able to follow the work plan as they had been instructed. While the 55-ft. reach of the man basket limited how far the victim could reach into the canopy of the tree, he was able to piece down the canopy by cutting through branches, which were an estimated 6 to 9 inches in diameter. However, at about 11 am, the victim decided to change course. The crew would not continue to methodically piece the tree down, it would attempt to bring down the upper two-thirds of the tree in two large pieces. The crewmembers did not check in with the general’s regional manager or the new subcontractor foreman before changing the plan. While cell phone reception was spotty in the ravine, contact was possible, either by driving approximately 7 minutes up the road, or by climbing up the ravine above the road.
The victim decided that he would fell each of the large spars by making cuts just above the split in the main trunk. This involved felling large sections of the remaining tree: the base of each spar was 16 to 18 inches in diameter, and extended upwards approximately thirty feet, before branching into what remained of the canopy (each linear foot of this spar weighed an estimated 134 lbs.1). In total, the sections were probably 50 to 60 feet in length. In an attempt to ensure that each spar would fall uphill onto the road, the crew tied a rigging line around the spar and attached it, via a redirecting pulley, to a mini-excavator located on the road. The excavator was to put initial tension on the spar, and then after the face-cut and back-cut had been made from the bucket truck, pull the spar over and up towards the road. It is not known how high up the spar the rigging line was attached.
The crew carried out this plan and the first spar fell, not onto the road (as was intended), but into the ravine. After some modifications, based on an assessment of what they thought had gone wrong, the crew was ready to fell the second spar using essentially the same strategy. The victim made the cuts from the bucket truck and then pulled the bucket back next to the near side of the bucket truck, parked approximately 10 to 15 feet from the base of the tree. The bucket was lowered to approximately 8 feet off the ground; the boom lift arm was folded back on itself, with its articulated joint in an elevated position.
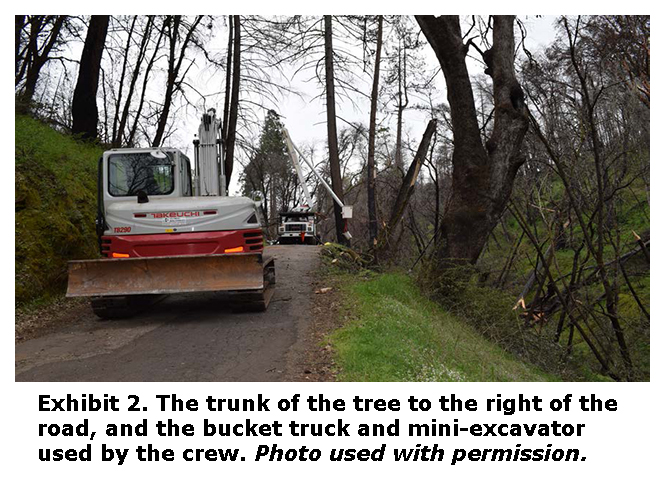
This time, as the excavator pulled, the spar initially moved as intended, but then abruptly changed direction and fell (at a right angle to the rigging line) towards the bucket truck. The upper part of the tree section struck the elevated boom arm and slid down the sloped arm towards the bucket, striking the victim and bouncing him out of the bucket (Exhibits 1 & 2). As he hung suspended from his body harness, his co-workers were able to reach and unclip him, and lay him on the road. The time was approximately 11:10 am.
The monitors and crew members began CPR immediately and took turns until the emergency medical services arrived. Witnesses were able to find spots on the hillside above the road that had cell phone reception, and five calls were placed to the 911 dispatcher. When emergency medical services arrived, they took over CPR. At approximately 12:11 pm, the paramedics conferred by phone with a physician, and the victim was pronounced dead at the scene.
Cause of Death
The cause of death, according to the death certificate, was blunt impact Injuries of head and torso.
Recommendations
CA/FACE concluded that organizations involved in tree-felling operations should take the following steps to prevent similar incidents:
Recommendation #1: Tree-felling contractors should ensure that each crew includes, and is led by, a person with substantial experience in tree felling.
Discussion: In this incident, the victim had only 3½ years of miscellaneous experience in the tree industry, and the oldest person on the crew was 25 years old. The victim may not have had the knowledge and experience needed to assess the best method to fell the tree and discern the risks involved in changing the original plan. Contractors, when constituting a crew, should ensure that it includes, and is led by, a person with substantial experience. This will help ensure not only a consistent adherence to safe practices, but continuing opportunities for on-the-job training. Had there been an experienced person leading this crew, he/she likely would not have chosen to fell the tree in an unsafe manner, and the fatality would have been prevented.
Recommendation #2: Tree-felling contractors should ensure that all supervisors are certified in tree-felling safety by an organization such as the Tree Care Industry Association (TCIA) or the International Society of Arboriculture (ISA). In addition, government agencies, utilities, and other project customers should include bid language requiring that all supervisors be certified in tree-felling safety by one of these organizations.
Discussion: In this incident, the supervisor was not certified in tree-felling safety. The crew was instructed to piece down the tree in sections, a method that was altered by the victim while the work was in progress. After altering the original work plan, the victim did not cradle the bucket truck boom and move the truck back a safe distance. Evidence suggests that the crew had not been clearly instructed to check in with their supervisor before changing the tree-felling plan, and had deviated from the original tree-felling plan on previous occasions. This suggests the lack of a robust safety culture with established practices of training, clear communication, adherence to safe work practices, adequate direct supervision, and consistent, impartial disciplinary action. Trade-specific safety training for all supervisors would help ensure a stronger safety culture in tree-felling projects. This is best attained by certification in tree-felling safety from the Tree Care Industry Association (TCIA) or the International Society of Arboriculture (ISA). This can be assured by bid language requiring that all supervisors possess this certification. Had there been adequate, well-trained safety supervision of the victim and his crew, it is more likely that safe practices would have been implemented and this fatality prevented.
Recommendation #3: Tree-felling crews should always be able to readily communicate with their supervisor and medical emergency services. If cell phone reception is not reliable, the employer should issue the crew a satellite phone.
Discussion: In this instance, the crew was working along a road in a steep creek ravine and had spotty cell phone reception. It is possible that the lack of reliable reception deterred the crew from attempting to contact their supervisor prior to abandoning the original tree-felling plan. Adequate supervision means, in part, that crews should be able to readily communicate with their supervisor at all times. In addition, it is very important for crews to be able to readily and reliably contact emergency medical services in the event of an injury, snake bite, allergic reaction, or heat illness. This is required by Cal/OSHA regulations Title 8, §3400, Medical Services and First Aid, and Title 8 §3395, Heat Illness Prevention. In this incident, co-workers were able to find spots on the hillside above the road that had cell phone reception, and five calls were placed to the 911 dispatcher. However, it is quite possible that contact with the 911 dispatcher could have been significantly delayed by relying solely on the spotty reception of personal cell phones.
Footnotes
1 ANSI Z133-2017, American National Standard for Arboricultural Operations—Safety Requirements, Annex E.References
ANSI Z133.-2017, American National Standard for Arboricultural Operations—Safety Requirements.
California Code of Regulations, Title 8, Section §3400, Medical Services and First Aid. (see: https://www.dir.ca.gov/title8/3400.html)
California Code of Regulations, Title 8, Section §3395, Heat Illness Prevention. (see: https://www.dir.ca.gov/title8/3395.html)
Exhibits

Case Report: 17CA004
Peter Scholz, CIH, FACE Investigator
Robert Harrison, MD, MPH, FACE Project Officer
Laura Styles, MPH, Research Scientist
September 5, 2018
FATALITY ASSESSMENT AND CONTROL EVALUATION PROGRAM
The California Department of Public Health, in cooperation with the Public Health Institute and the National Institute for Occupational Safety and Health (NIOSH), conducts investigations of work-related fatalities. The goal of the CA/FACE program is to prevent fatal work injuries. CA/FACE aims to achieve this goal by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact. NIOSH-funded, state-based FACE programs include: California, Kentucky, Massachusetts, Michigan, New York, Oregon, and Washington.
Additional information regarding the CA/FACE program is available from:
California FACE Program
California Department of Public Health
Occupational Health Branch
850 Marina Bay Parkway, Building P, Third Floor
Richmond, CA 94804
www.cdph.ca.gov/face