
NIOSH FACE Report - Maintenance Worker Struck by Forklift Carriage—Tennessee
-
Fatality Assessment and Control Evaluation (FACE) Program Reports
The National Institute for Occupational Safety and Health’s (NIOSH) Fatality Assessment and Control Evaluation (FACE) Program and State FACE Programs study fatal workplace injuries and prepare reports with recommendations to prevent similar injuries. The following are links to all of the items in this collection:
Documents
- Kentucky FACE Report: Commercial Roofer Falls 30 Feet Through a Skylight While Installing Roof Insulation
- Fatal Occupational Injuries in Massachusetts 2008-2013
- Fatality Assessment & Control Evaluation (FACE) Program
- Washington FACE Report: Glazier Foreman Falls From Stepladder
- Preventing Construction Falls Toolkit
- Hazard Alert: Pedestrian Workers Killed by Forklifts
- Keep Employees in Motor Vehicles Safe
- New York FACE Brochure
- Washington FACE Report: Construction Laborer Falls When Ladder Breaks
- Washington FACE Report: Pipelayer Dies when Trench Wall Collapses
- Washington FACE Report: Carpenter Falls 60 Feet from Bridge Concrete Form
- Washington FACE Report: Foreman and Laborer Fall when Aerial Lift Struck by Vehicle
- Washington FACE Report: Framer Falls 18 Feet while Sheathing Roof
- New York FACE Report: Mechanic Electrocuted when a Mobile Light Tower Contacted Powerline
- New York FACE Report: Two Construction Workers Fatally Crushed when Cement Formwork Collapsed
- Kentucky FACE Report: Construction Laborer Killed in Trench Collapse while Taking Grade Measurements
- California FACE Report: A Heating, Ventilaton and Air Conditioning (HVAC) Contractor Dies when He Falls through a Skylight
- Massachusetts FACE Report: Carpenter Fatally Injured after Falling from an Extension Ladder
- Massachusetts FACE Report: Laborer Fatally Injured after Falling from a Home under Construction
- Oregon FACE Report: Worker Falls When Ladder Slips
- Michigan FACE Information Sheet: Look for Mobile Equipment Blind Spots
- Oregon FACE Report: Collapsed roof trusses kill carpenter foreman
- Washington FACE Report: Roofer Falls 19 Feet from Roof
- Hazard Alert: Plan. Provide. Train. Prevent Fall Injuries & Deaths
- Kentucky FACE Report: 19-Year-Old Construction Laborer Crushed in Trench Collapse While Laying Sewage Pipe
- Kentucky FACE Report: Construction Flagger Struck and Killed in Two-Lane Highway Work Zone
- Kentucky FACE Report:Temporary Electrician Helper Steps into Unguarded Elevator Shaft and Dies
- Fatality Narrative: Roofing Contractor Falls 25 Feet From Church Roof
- Kentucky FACE Report: Construction Siding Subcontractor Installer Killed when Oversized Scaffolding Platform Destabilized and Telescopic Forklift Overturned
- NIOSH FACE Report - Maintenance Worker Struck by Forklift Carriage—Tennessee
- Kentucky Hazard Alert: Roofing and Construction Workers Killed Due to High Winds
- Poster: Secure it to move it!
- Oregon FACE Report: Crane Operator Killed By Falling Steel Beam
- New Jersey FACE Report: Mechanic Dies After Being Crushed Under Electrical Cabinet
- New Jersey FACE Report: Plant Manager Crushed to Death Under Fallen Pile of Steel Beams
- NIOSH FACE Report: Hispanic worker falls from residential roof
- Oregon FACE Report: Construction worker died after falling 20-25 feet from a pump-jack scaffold
- FACE Fact Sheet: Prevent Construction Falls from Roofs, Ladders, and Scaffolds
- Construction Fatality Narrative: Roofer Falls 18 Feet from Wet House Roof
- Construction Worker Killed when Trench Collapsed, Oregon
- A Tree Trimmer is Electrocuted While Trimming a Palm Tree
- A Tree Feller Dies When Struck By a Tree Limb While Felling a Fire-Damaged Tree
- Concrete Finisher Electrocuted When Bull Float Contacted an Energized Power Line
- Warehouse Worker Crushed by Forks of Laser Guided Vehicle
Summary Statement
The NIOSH FACE program report examines a fatal accident involving use of improper procedures during forklift carriage repairs. Lack of specific written maintenance procedures and lack of job and task hazard analysis and not following manufacturer and internal safety guidelines for repair and maintenance of equipment were the primary contributing factors to this fatality.
July 22, 2016
SUMMARY
On February 28, 2014, a 51-year-old maintenance worker was crushed by the forks of a forklift he was repairing. At the time of the incident, the maintenance worker was working below the elevated forks, replacing a hydraulic seal on the forklift carriage lift mechanism while the carriage and forks were supported by resting the fork tips on the edge of a shipping container. The forklift operator was standing next to the forklift. As the maintenance worker tightened a hydraulic fitting, the fork tips slipped off the container edge. The carriage and forks fell, striking his head and pinning him underneath. The forklift operator radioed to call 911. Emergency medical services dispatched to the incident, and the maintenance worker was transferred to the hospital where he succumbed to his injuries.
CONTRIBUTING FACTORS
Key contributing factors identified in this investigation include:
- Lack of specific written maintenance procedures for hydraulic seal replacement
- Working under an elevated, unsecured forklift carriage
- Lack of job and task analysis to identify the hazard
- End of work shift
RECOMMENDATIONS
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
- Establish an equipment maintenance and inspection program and ensure workers follow manufacturer and company safety guidelines for repair and maintenance of equipment.
- Develop, implement, and train workers on proper hazardous energy control procedures, specifically unsecured elevated loads.
- Ensure only trained, authorized personnel maintain, repair, adjust, and inspect powered industrial trucks (e.g., forklifts) and provide periodic refresher training.
- Complete job and task hazard analyses and train workers on the results of these analyses.
Fatality Assessment and Control Evaluation (FACE) Program
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1982, NIOSH initiated the Fatality Assessment and Control Evaluation (FACE) Program. FACE examines the circumstances of targeted causes of traumatic occupational fatalities so that safety professionals, researchers, employers, trainers, and workers can learn from these incidents.The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent occupational deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under the FACE program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/face/ or call toll free at 1-800-CDC-INFO (1-800-232-4636).
INTRODUCTION
At 2:30 p.m. on February 28, 2014, a 51-year-old maintenance worker was fatally injured when he was struck by the carriage of a forklift he was repairing. On March 5, 2014, the Tennessee Department of Labor and Workforce Development/Occupational Safety and Health Division (TOSHA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research, of the incident. On September 11, 2014, a health scientist conducted an investigation of the fatality and reviewed circumstances of the incident with the investigating safety compliance officer from the Tennessee Department of Labor (TNDOL). Photographs of the incident site taken by the volunteer fire department and witness statements taken by TNDOL were reviewed.
EMPLOYER
The employer was a water bottling company that employed 400 workers nationwide. The employer had 82 workers on-site and had been in business in this location since 1998. The parent company has been in business since 1990 and has eight plants throughout the country.
WRITTEN SAFETY PROGRAMS and TRAINING
At the time of the incident, according to TOSHA, the employer had a comprehensive written occupational safety and health program, which included HAZCOM, lockout/tagout, bloodborne pathogens, and forklift operator training. Training was given at the time of employment, then annually, or when workers changed positions; forklift training was refreshed every 3 years. Personal protective equipment was provided by the employer and included hard hats and steel-toe boots. The employer’s safety program included a policy of not working under unsecured loads or dismounting a forklift without lowering the forks.
WORKER INFORMATION
The maintenance worker typically worked from 7:00 a.m. to 3:30 p.m. At the time of the incident, the maintenance worker was wearing a hard hat and steel-toe boots. The maintenance worker had completed lockout/tagout training in 2008 and training on Toyota hydraulic power-train systems in 2003. The maintenance worker had a discipline report in 2013 where he had been advised to not work under an unsecured raised load.
INCIDENT SCENE
The forklift was being repaired outside near the maintenance shop in a concrete paved yard. A CONEX shipping container was also located outside with a pallet on the ground next to it. The pallet measured 48 inches wide and 12 inches tall. A steel plate and a tractor-trailer door were stacked on the pallet (Photo 1). The pallet with steel plate and tractor trailer door, which was on the ground next to the shipping container, was approximately 51 inches long, and the shipping container was 101 inches tall. The pallet was 7 inches from the mast of the forklift. The forks were 58 inches long (Diagram 1). This allowed only the tips of the forks to rest on the shipping container. After the incident, scratches were observed on the side of the shipping container approximately 1 inch from the top edge where the forks had rested (Photo 2).

Photo 1. Incident scene, pallet with material
on the ground; arrow indicates forklift
involved. (Photo courtesy of TOSHA)
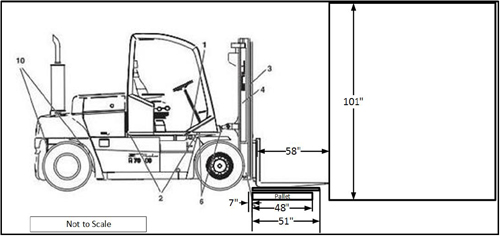
Diagram 1. Forklift, pallet, and shipping container
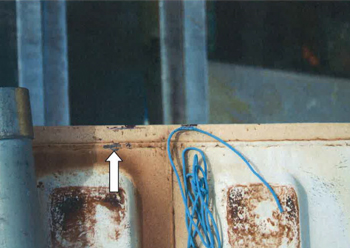
Photo 2. Arrow indicates scratches on shipping
container. Photo courtesy of TOSHA
EQUIPMENT
The forklift involved in the incident was a liquid petroleum gas powered, Toyota Model 8FGU32 with a 6,500-lb capacity, three-stage (FSV) mast, and dual load attachment. The dual load attachment on the carriage of the lift measured 58 inches from the front edge of the mast to the tips of the forks.
WEATHER
The weather at the time of the incident was approximately 50 degrees Farenheit, 22% humidity, and 5 mph wind speed. Weather is not believed to have been a factor in this incident [Weather Underground 2014].
INVESTIGATION
Toward the end of the shift on February 28, 2014, the forklift operator noticed the forklift had a hydraulic leak. The forklift operator notified the maintenance worker that the forklift was leaking hydraulic fluid from the mast area of the forklift. The maintenance worker saw the leak and instructed the operator to drive the forklift to the shipping container so he could further examine the problem. The maintenance worker instructed the operator of the forklift to elevate the carriage and set the forks on top of a shipping container. The operator verified the forklift was positioned as the maintenance worker wanted it, then set the emergency brake on the forklift, turned off the forklift, and exited the forklift. The pallet on the ground with the steel plate and tractor-trailer door on it prevented the forklift operator from moving closer to the shipping container and allowed only the tips to be placed on the top of the container side.
The maintenance worker walked under the elevated forks, kneeled down, and proceeded to examine the hydraulic cylinder. The maintenance worker determined the leak was coming from the hydraulic hose fitting into the hoist cylinder (Photo 3). The maintenance worker and operator went to retrieve a replacement O-ring from the maintenance shop. They returned with the O-ring, and the maintenance worker positioned himself under the forks and began to replace the O-ring. The maintenance worker asked the operator to step out of the way while he repaired the forklift. The maintenance worker sat down on a bucket under the elevated forks, drained the hydraulic fluid, removed the damaged O-ring, installed a new O-ring and began to replace the hose fitting. When the maintenance worker turned the wrench to tighten the fitting, the forks of the forklift were dislodged and slipped off the shipping container. The carriage on the forklift mast fell and struck the maintenance worker in the back of the head, pinning him between the tractor trailer door on the pallet, which was under his feet, and the carriage of the forklift. The operator radioed for 911 and emergency medical services dispatched to the incident. The maintenance worker was then transferred to the hospital where he succumbed to his injuries.

Photo 3. Right arrow indicates repair location
on mast; left arrow indicates where the carriage
hit the worker. (Photo courtesy of TOSHA.)
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following unrecognized hazards as key contributing factors in this incident:
- Lack of specific written maintenance procedures for hydraulic seal replacement
- Working under an elevated, unsecured forklift carriage
- Lack of job and task analysis to identify the hazard
- End of work shift
CAUSE OF DEATH
According to TOSHA, the cause of death was multiple crushing injuries to the head and chest.
RECOMMENDATIONS/DISCUSSION
Recommendation #1:
Employers should establish an equipment maintenance and inspection program and ensure workers follow manufacturer and company safety guidelines for repair and maintenance of equipment.
Discussion: The American National Standards Institute (ANSI) recommends that maintenance and inspection of all powered industrial trucks shall be performed in conformance with the manufacturer’s recommendations before working on or under the load-engaging means (e.g., the forks), inner mast, or chassis [ANSI 2012]. OSHA mandates that no person shall be allowed to stand or pass under the elevated portion of any truck, whether loaded or empty [Powered industrial trucks 2006]. ANSI B56.1 1969 Section 6 603B states, “Do not stand or pass under the elevated portion of any truck, whether loaded or empty.” In this incidence, the maintenance worker was working under unsecrured elevated forklift forks.
The employer had a policy of not working under unsecured raised loads or dismounting the forklift without lowering the forks. The maintenance worker had been advised on a previous occasion not to work under the unsecured raised carriage of a forklift and to use the vehicle lift in the mechanic shop to raise and support the carriage. The employer did not have specific written procedures for replacement of O-rings on the forklift carriage. The maintenance manual for the forklift recommended the mast be secured using a hoist and sling. The inner mast should be further supported with wooden blocks placed at the bottom of the mast then secure the blocks to the outer mast with tape [Toyota 2010]. The Association of Equipment Manufacturers recommends removing the fork attachment and installing an appropriate support device before raising the mast carriage [AEM 2009]. Supporting the elevated mast carriage with jack stands ensures stability of the carriage, especially when work has to be performed under the carriage. Jack stands are designed to support a vertical loads so it is essential that the jack is placed on a level surface [CAFACE 2001, 2003]. Had the mast carriage been secured before beginning work, this incident might have been prevented.
Recommendation #2:
Employers should develop, implement, and train workers on proper hazardous energy control procedures, specifically unsecured elevated loads.
Discussion: Employers should develop hazardous energy control programs for all equipment requiring maintenance. This program should include hazardous energy control procedures, employee training, and periodic inspections. Before any employee performs any maintenance on a machine or equipment, inspections should ensure that the unexpected energizing, startup, or release of stored energy does not occur and cause injury [The Control of Hazardous Energy 2011]. Forms of hazardous energy include kinetic, potential, electrical, and thermal [NIOSH 1999]. In this incident, the potential energy of the raised forklift carriage was released when the fork tips slipped off of the container, allowing the carriage to fall.
Procedures should be developed, documented, and utilized for the control of potentially hazardous energy when employees are engaged in servicing or maintenance of a machine or equipment [The Control of Hazardous Energy 2011]. This procedure should have enough detail for authorized employees to have a clear understanding of the energy control measures required so that they may follow the procedural steps to effectively control all types and forms of hazardous energy. A documented written energy control procedure is necessary. The energy control procedures should clearly and specifically outline the scope, purpose, authorization, rules, and techniques that will be used to control hazardous energy sources, as well as the means that will be used to enforce compliance. At a minimum, these procedures should also include the following elements:
- A specific statement of the intended use of the procedures.
- The specific procedural steps for shutting down, isolating, blocking, and securing machines or equipment to control hazardous energy.
- The specific procedural steps for placement, removal, and transfer of lockout/tagout devices and the responsibility for them.
- The specific requirements for testing a machine to determine and verify the effectiveness of lockout/tagout [OSHA 2008].
Before beginning service or maintenance, the following steps should be accomplished in sequence and according to the specific provisions of the employer’s energy-control procedure:
- Prepare for shutdown.
- Shut down the machine.
- Disconnect or isolate the machine from the energy source(s).
- Apply the lockout or tagout device(s) to the energy-isolating device(s).
- Release, restrain, or otherwise render safe all potential hazardous stored or residual energy. If a possibility exists for accumulation of hazardous energy during the servicing, regularly verify that such energy has not accumulated to hazardous levels.
- Verify the isolation and de-energization of the machine [OSHA 2002a].
At the time of the incident, the employer did not have specific lockout/tagout procedures to prevent the potential release of energy from a falling forklift carriage. After this incident, the employer developed a lockout/tagout procedure that included training on removing the fork attachment and using jack stands to support the carriage before relieving hydraulic pressure from the mast lift cylinder.
Recommendation #3:
Employers should ensure only trained, authorized personnel maintain, repair, adjust, and inspect powered industrial trucks (e.g., forklifts) and provide periodic refresher training.
Discussion: OSHA mandates that any power-operated industrial truck not in safe operating condition shall be removed from service. All repairs shall be made by authorized personnel [Powered industrial trucks 2006]. In this incident, the equipment operator recognized the forklift was leaking hydraulic fluid and notified the maintenance personnel, who quickly put the forklift out of service. The employer had a forklift operator-training program and sent maintenance personnel to forklift maintenance training. The maintenance worker had received hydraulic power train systems training in 2003. The company providing the maintenance training offered courses on engines, electrical systems, hydraulic power train systems, class II forklifts, 7-series electric lift trucks, and electronic engine control systems. When talking with the plant manager on a previous occasion, the maintenance worker stated that, based on the training received in 2003, the forks needed to be elevated 3 feet to service the main cylinder. In 2008, the Association of Equipment Manufactures produced a guidance document, Rough Terrain Forklift Trucks Safety Manual for Operating and Maintenance Personnel [AEM 2009]. This document recommends removing the fork attachment before raising the mast carriage, then install an appropriate support device. Employers should provide refresher training, similar to forklift operator training, or more often if necessary.
Recommendation #4:
Employers should complete job and task hazard analyses and train workers on the results of these analyses.
Discussion: Employers should conduct job and task hazard analyses for all employees in all work areas and for all job tasks. A job hazard analysis focuses on job tasks in an attempt to identify hazards before they occur and focuses on the relationship between the worker, the task, the tools, and the work environment. A job hazard analysis should begin by reviewing the work activities or tasks for each employee. Each task is further examined for mechanical, electrical, chemical, or any other hazard the worker may encounter. After identifying uncontrolled hazards, the employer should take steps to eliminate or reduce the hazards. For a job hazard analysis to be effective, management should follow through to correct any uncontrolled hazards identified, train the employees on the proper hazard mitigation strategy, and discipline if the hazard mitigation strategies are not followed [OSHA 2002b].
DISCLAIMER
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites. All web addresses referenced in this document were accessible as of the publication date.
REFERENCES
AEM [2009]. Rough terrain forklift trucks safety manual for operating and maintenance personnel. Milwaukee, WI: Association of Equipment Manufacturers, FORM RTF-0907.
ANSI [2012]. ANSI B56.1-2012 Safety standard for low lift and high lift trucks, powered and nonpowered industrial trucks. Washington, DC: American National Standards Institute, Section 7, http://www.itsdf.org/docs/standards/ITSDF%20B56-1-2012-rev-08-15-12.pdf.
CAFACE [2001]. A mechanic dies when struck in the head by a forklift that slipped off a jack. Richmond, CA: California Department of Health Services, Occupational Health Branch, http://www.cdc.gov/niosh/face/stateface/ca/01ca001.html.
CAFACE [2003]. A maintenance mechanic died when the forklift he was working on slipped off a jack and fell on him. Richmond, CA: California Department of Health Services, Occupational Health Branch, http://www.cdc.gov/niosh/face/stateface/ca/03ca005.html.
The control of hazardous energy (lockout/tagout). 29 CFR 1910.147 (2011), https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=9804.
NIOSH [1999]. NIOSH alert: preventing worker deaths from uncontrolled release of electrical, mechanical, and other types of hazardous energy. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 99–110, http://www.cdc.gov/niosh/docs/99-110/pdfs/99-110.pdf.
OSHA [2002a]. Control of hazardous energy lockout/tagout. Revised. Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration, OSHA 3120, https://www.osha.gov/Publications/osha3120.pdf.
OSHA [2002b]. OSHA 3071 Job hazard analysis. Revised. Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration, OSHA 3120, https://www.osha.gov/Publications/osha3071.html.
OSHA [2008]. OSHA Directive CPL 02-00-147 The control of hazardous energy—enforcement policy and inspection procedures. Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration, https://www.osha.gov/OshDoc/Directive_pdf/CPL_02-00-147.pdf.
Powered industrial trucks. 29 CFR 1910.178 (2006), https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=9828.
Toyota [2010]. Toyota repair manual 8FGU32. Columbus, IN: Toyota Material Handling Company, a Division of Toyota Industries Corporation, Pub. No. CU066, Section 12-8.
Weather Underground [2014]. Weather history for KRZR. Atlanta, GA: The Weather Channel Interactive, Inc., http://www.wunderground.com/history/airport/KRZR/2014/2/28/DailyHistory.html.
INVESTIGATOR INFORMATION
This investigation was conducted by Jennifer E. Lincoln, Health Scientist, Fatality Investigations Team, Surveillance and Field Investigation Branch, Division of Safety Research.
ACKNOWLEDGEMEMENT
The NIOSH FACE Program and the health scientist would like to acknowledge the compliance officer and staff of the Tennessee Department of Labor and Workforce Development, Occupational Safety and Health Division and Michael Fiore from the Massachusetts FACE Program.
__________________________________________ Date: ________________
Jennifer E. Lincoln, Health Scientist
Fatality Assessment and Control Evaluation Program
Surveillance and Field Investigations Branch
Division of Safety Research
_____________________________________________ Date: ________________
Nancy Romano, Project Officer
Fatality Assessment and Control Evaluation Program
Surveillance and Field Investigations Branch
Division of Safety Research
_____________________________________________ Date: ________________
Paul H. Moore, Chief
Fatality Investigations Team
Surveillance and Field Investigations Branch
Division of Safety Research
_____________________________________________ Date: ________________
John Myers, Chief
Surveillance and Field Investigations Branch
Division of Safety Research
_____________________________________________ Date: ________________
Tim Pizatella, Deputy Director
Division of Safety Research

FACE - Fatality Assessment and Control Evaluation Program
Division of Safety Research
1095 Willowdale Road
Morgantown, West Virginia 26505
(304) 285-5916