
Summary Statement
A broad collection of tables and charts covering health and safety in the U.S. construction industry, as well as considerable economic and training data.
2007
Section 50: Utilization of Health Services among Construction Workers
Utilization of health care services varies among construction workers. Two factors that can influence utilization patterns are whether or not the worker has health care coverage and whether or not the worker is of Hispanic ethnicity.
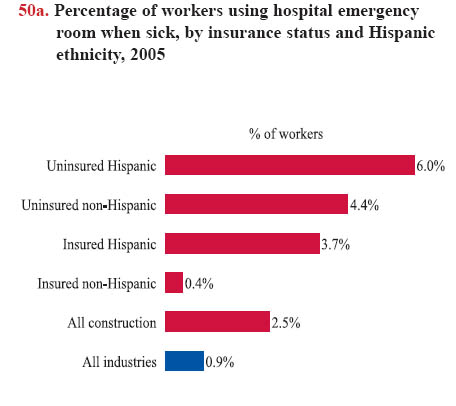
Construction workers without health insurance, regardless of ethnicity, are less likely to have a consistent location for receiving health care services and are more apt to use emergency rooms than workers who are insured. In 2005, 6.0% of uninsured Hispanics reported that they visited the hospital emergency room as "a usual place of health care" when sick compared with only 3.7% of Hispanics with health insurance (chart 50a). This proportion among uninsured Hispanic construction workers using the ER when ill was not only more than workers in all construction, but also considerably higher than the average for all industries.
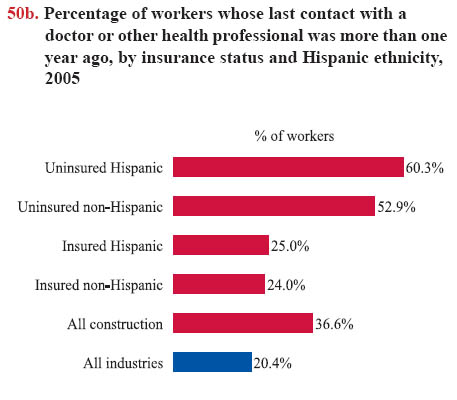
Having health insurance also affects frequency of care: construction workers without health insurance have fewer visits to a health provider. In 2005, 60.3% of uninsured Hispanic workers had not seen a doctor or health professional in more than 12 months (chart 50b). When the worker had insurance, the likelihood was cut in half: just 25% of insured Hispanics and 24% of white, non-Hispanics had not seen a health professional in over a year.
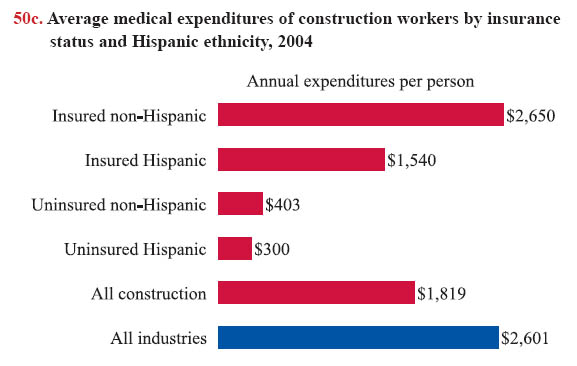
Another way to analyze health care utilization is to examine the amount of medical expenditures, or the payments made to health providers and institutions.1 Workers with insurance generally have higher medical expenditures than workers without insurance (chart 50c). For example, a Hispanic construction worker without insurance only used $300 for health care per year, less than one-fifth of medical expenditures for an insured Hispanic worker.
Low health insurance coverage among construction workers, especially Hispanics (see chart book page 26), is a large contributing factor to the disparities in health services. However, union members should be more likely to have access to health services than non-union workers because of high rates of health insurance coverage among union members in construction. Other factors, such as health status, age, family income, and gender, also can influence the use of health services. Lack of access to health care can delay health services and lead to poor health outcomes.
The data used for this page were obtained from the National Health Interview Survey (NHIS; see chart book page 46) and the Medical Expenditure Panel Survey (MEPS; see chart book pages 48 and 49). Although both the NHIS and MEPS collect similar information on health services, NHIS respondents were asked to recall events for the entire year during a single interview, while MEPS respondents were asked about medical events that occurred during the calendar year at three points in time. An important objective of the MEPS is to produce descriptive estimates of health care use, expenditures, and sources of payment, while the NHIS provides more detailed information on health behaviors. Because both NHIS and MEPS are based on self-reported information, it is possible that respondents in each of the surveys misclassified or inaccurately recalled the health services they used.
Download MS PowerPoint versions of Charts
1. Medical expenditures include payments from all sources to hospitals, physicians, other medical care providers, and pharmacies for services received for medical conditions reported by respondents. Sources include direct payments from individuals, private insurance, Medicare, Medicaid, workers' compensation, and miscellaneous other sources. Expenditures for hospital-based services include those for both facility and separately billed physicians' services. Over-the-counter drugs, alternative care services, or telephone contacts with medical providers are not included.
Note: All charts - "Non-Hispanic" is technically white, non-Hispanic.
Source: Charts 50a and 50b - National Center for Health Statistics, 2005 National Health Interview Survey (NHIS). Calculations by
CPWR Data Center.
Chart 50c - Agency for Healthcare Research and Quality, 2004 Medical Expenditure Panel Survey (MEPS). Calculations by
CPWR Data Center.
Back to Table of Contents