
Summary Statement
A broad collection of tables and charts covering health and safety in the U.S. construction industry, as well as considerable economic and training data.
2007
Section 46: Health Risk Factors and Chronic Illnesses Among Construction Workers
Cigarette smoking, obesity, diabetes, hypertension (high blood pressure), and high blood cholesterol are major risk factors for coronary heart disease.1 Cigarette smoking is also associated with a tenfold increase in the risk of dying from chronic obstructive lung disease.2 The adverse health effects from cigarette smoking account for nearly one of every five deaths in the United States, more than by all deaths from human immunodeficiency virus (HIV), illegal drug use, alcohol use, motor vehicle injuries, suicides, and murders combined.2
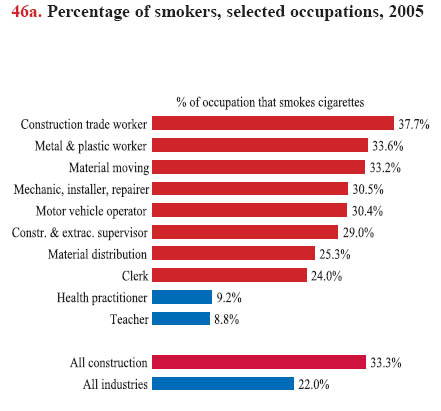
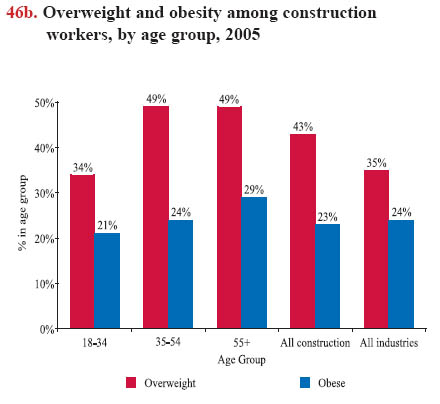
Although people are well aware that smoking is harmful, cigarette or tobacco smoking is still widespread, particularly among production (blue-collar) workers. In 2005, nearly 38% of workers in construction trades were current smokers, about 1.7 times that of all industries (chart 46a). The risk of chronic lung disease and cancer from smoking is increased among construction workers due to other hazardous respiratory exposures, including welding, silica and asbestos (see chart book page 43).Obesity also has been linked to stroke, diabetes, and several other chronic conditions. The prevalence of obesity among adults, as measured by a body mass index (BMI) rating (see Glossary), has doubled in the past two decades.3 In 2005, about two out of three (66%) construction workers were either overweight or obese, compared with 59% for all industries combined (chart 46b).
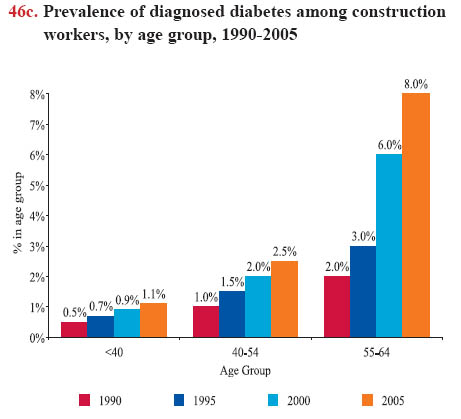
Diabetes is a serious chronic illness that greatly increases the likelihood of developing disabling health problems and is the sixth leading cause of death in the United States. The risk of diabetes increases with age. Approximately 10% of the U.S. population over age 40 and 21% of those age 60 or older have this disease. 4 During the last decade, the prevalence of diabetes dramatically increased among workers in construction trades, particularly in those over age 55 (chart 46c). Approximately 7% (21 million) of the entire U.S. population have diabetes; of those, an estimated 6.2 million people are undiagnosed.5 According to a medical screening program among construction workers, about half of the diabetics identified by the screening did not know that they had diabetes.6
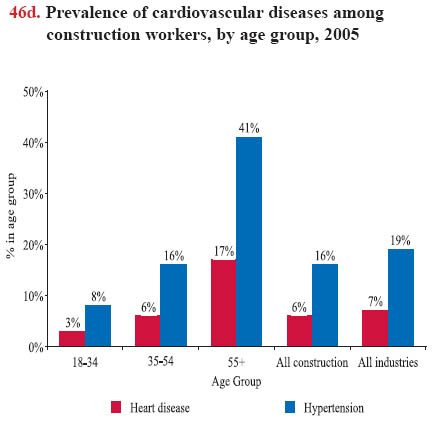
High blood cholesterol and hypertension are very common among older adults. About 41% of construction workers age 55 and older were diagnosed with hypertension in 2005, and 35% of this age group reported they were told their blood cholesterol level was high (chart 46d).7 High level of blood cholesterol and hypertension are closely associated with a higher prevalence of heart disease among older construction workers.
Heart disease is the leading cause of death in the United States and a major cause of disability. Almost 700,000 people die from heart disease each year, accounting for 29% of all U.S. deaths.8 The prevalence of heart disease for construction (6%) is slightly lower than that for all industries (7%; chart 46d). Construction workers are younger on average than workers in other industries, and the high physical demands of the work will cause many construction workers with heart disease to leave the workforce (the healthy worker effect). The data may underestimate the true prevalence; construction workers with heart disease are 60% more likely to retire on disability than other construction workers.9
Worksite health promotion programs have proven to be effective in other industries, but novel approaches to promoting healthful behaviors are needed in construction, where workers change job sites frequently and thus may have limited access to worksite health promotion efforts. Since programs tailored specifically for construction workers to reduce smoking were successful, 10, 11 similar efforts should continue and target other health outcomes, such as reducing hypertension and diabetes in the construction worker population. An important characteristic of these successful programs was that information about smoking cessation was integrated into training about toxic exposures at work and/or presented in a way that was tailored for a blue-collar population. A systems approach, focusing on developing workplace policy and practices to promote health rather than simply focusing on individual behavior, appears to be more effective.10, 11
Download MS PowerPoint versions of Charts
1. American Heart Association, Cigarette Smoking and Cardiovascular Diseases, http://www.americanheart.org (Accessed November 2007).
2. Center for Disease Control and Prevention (CDC), Health Effects of Cigarette Smoking, http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm (Accessed November 2007).
3. Allison A. Hedley, Cynthia L. Ogden, Clifford L. Johnson, Margaret D. Carroll, Lester R. Curtin, and Katherine M. Flegal. 2004. Prevalence of Overweight and Obesity among U.S. Children, Adolescents, and Adults, 1999-2002. The Journal of the American Medical Association, 291:2847- 2850.
4. American Diabetes Association, Total Prevalence of Diabetes & Pre-diabetes, www.diabetes.org/diabetes-statistics/prevalence.jsp (Accessed November 2007).
5. Centers for Disease Control and Prevention, http://www.cdc.gov/diabetes/statistics/prev/national/figpersons.htm (Accessed November 2007).
6. CPWR findings from a medical screening program of over 10,000 pulmonary function tests and chest X-rays of current and former construction workers at Department of Energy nuclear weapons facilities 1996-2006, updated through 2007 (unpublished data).
7. National Center for Health Statistics, 2003 National Health Interview Survey. Calculations by CPWR Data Center.
8. American Heart Association. 2005. Heart Disease and Stroke Statistics – 2005 Update. Dallas, TX: American Heart Association.
9. Mikael Stattin and Bengt Järvholm. 2005. Occupation, Work Environment, and Disability Pension: A Prospective Study of Construction Workers. Scandinavian Journal of Public Health, 33(2):84-90.
10. Glorian Sorensen, Elizabeth Barbeau, Anne Stoddard, Mary Hunt, Roberta Goldman, Ann Smith, Angela Brennan, and Lorraine Wallace. 2007. Tools for Health: The Efficacy of a Tailored Intervention Targeted for Construction Laborers. Cancer Causes and Control, 18(1):51-59.
11. Knut Ringen, Norman Anderson, Tim McAfee, Susan M. Zbikowski, and Donald Fales. 2002. Smoking Cessation in a Blue-Collar Population: Results from an Evidence-Based Pilot Program. American Journal of Industrial Medicine, 42(5):367-377.
Note:
Chart 46b - Overweight is a body mass index (BMI) between 25 and 29.9. A person is obese with a BMI of 30 or higher. See Glossary for a full description of BMI or go to http://www.nhlbisupport.com/bmi/ (Accessed November 2007).
Source:
Charts 46a, 46b, and 46d - National Center for Health Statistics, 2005 National Health Interview Survey. Calculations by CPWR Data Center.
Chart 46c - Data supplied by Duke University from medical claims file for one Health and Welfare Fund.
Back to Table of Contents