
A Safety & Health Practitioner's Guide to Skin Protection
-
Guide to Skin Protection
The following are links to all of the items in this collection:
Summary Statement
An in-depth discussion of skin protection from exposure to cement, including causes, prevention, and training materials to be used with workers. Part of a collection. Click on the 'collection' button to access the other items.
2000
This material is supported in part with funds from the National Institute for Occupational Safety and Health (NIOSH) through CPWR – Center for Construction Research and Training to a consortium of CPWR, the Operative Plasterers & Cement Masons International Association, and FOF Communications. Researched, written, and produced by FOF Communications.
The material does not necessarily reflect the views or policies of NIOSH. Mention of trade names, commercial products or organizations does not imply endorsement by NIOSH, the U.S. Government, CPWR, OPCMIA, or FOF Communications.
The Occupational Safety and Health Act of 1970 makes the employer responsible for providing a safe and healthful workplace that is free of recognized hazards.
© 1999, 2000 FOF Communications
Table of Contents
Preface:
Printer-Ready
Pull Outs:
| Worker Safety Pamphlet | |
| Best Practices Checklist | |
| Symptoms Questionnaire |
Preface
If you are responsible
for protecting the safety and health of workers who use wet portland cement
products—concrete, mortar, plaster, grout, stucco, terrazzo, or other
products, this guide is for you. It will help you prevent skin problems
from cement.
Development of this guide was supported by the National Institute for
Occupational Safety and Health through a CPWR Consortium on Preventing
Contact Dermatitis. Consortium partners are CPWR – Center for Construction Research and Training, the Operative Plasterers & Cement Masons International Association,
and FOF Communications. The guide was researched, developed, and produced
by FOF Communications.
The consortium steering committee includes: David Hinkamp, MD; Boris Lushniak,
MD, of NIOSH; Jon Mullarky and Greg Vickers of the National Ready Mixed
Concrete Association; William Schell of the Operative Plasterers & Cement
Masons International Association; John Sullivan, Jr., P.E., of the American
Portland Cement Alliance; Azita Mashayekhi of the International Brotherhood
of Teamsters, and Eileen Betit of the International Union of Bricklayers
& Allied Craftsworkers.
The consortium has been instrumental in focusing the cement industry on
skin problems and in disseminating innovative protective measures such
as the use of buffers and other neutralizing agents. The consortium supported
a Physician Alert brochure to help Portland cement products workers talk
with their doctors; the Save Your Skin booklet on glove wear; An Employer's
Guide to Skin Protection; a Tool Box Pamphlet; a worker classroom training
course; a training evaluation study; jobsite visits for pH testing of
surface skin and rinse water; a stakeholder symposium, and a professional
advisory group meeting on the development of this handbook.
To learn more, visit NIOSH at www.cdc.gov/niosh
or CPWR – Center for Construction Research and Training at www.cpwr.com
or call the NIOSH Technical Information Branch (800-356- 4674) or CPWR
(301-578-8500).
Recognizing
Skin Problems
Ted Jason' s eight-year
old daughter got a painful rash that would not go away. The Jasons took
her to several doctors. They applied ointments. They washed her sore skin
with prescribed soaps. Nothing they did made a difference.
Then Ted took a course on preventing dermatitis from Portland cement .
He learned to measure the pH of the surf aces of his skin, his boots,
and his car interior.
Ted found out that alkaline cement residue from his work had contaminated
his life in a way he had never before appreciated. He realized his daughter
had been exposed.
So Ted began following the tips given in the course. He cleaned his car
interior and began removing his work clothes before getting into it .
He switched to pH-neutral soap for his family. Within a few weeks, his
daughter's skin problem was gone—and so was his.
‘Dermatitis Won't Kill You'
What does Ted Jason' s story tell us about many port land cement products
workers? Too often, they may feel they must accept their skin problems
as part of the job. Ted became serious about treating dermatitis only
when his own daughter got a skin problem.
Skin problems from cement are widespread. Unfortunately, problems are often tolerated as part of the price of the work in some trades. Our tolerance permits the high rates of occupational skin problems in the United States to continue. A change in attitude is needed.
As a safety & health practitioner, you may find that you too hold many of the more traditional assumptions about how to prevent occupational skin problems.
If you believe skin protection is fundamentally a matter of getting workers into the proper gloves, then you will find much in this guide that is innovative and thought-provoking.
One of your challenges is to convince cement products workers that it is possible for them to prevent occupational skin problems. But first, they - and you--must recognize when skin problems exist. Often, rashes and other symptoms are downplayed or overlooked as a prelude to chronic disease.
A central challenge
is motivation. Here the health impact on family members and partners 1
may be key. Workers are motivated to take protective measures when they
believe it protects their children. 2 Other key motivations
include comfort and availability and a belief that employers, fellow workers,
and union representatives support their actions.2
 |
Dry skin or irritation. Wet cement dries and irritates skin. |
As a safety & health practitioner, you can take many actions in support of worker protection. In addition to educating workers, you can educate employers. You can work to create an environment in which the individual worker’s decision to adopt protection is reinforced by social influences and in which protections are readily available and easy to use.
As a safety &
health practitioner, you can help workers choose the right protective
measures, you can convince employers to take the best protective actions,
and you can keep both groups continually motivated so that incremental
progress will be made.
Portland cement products workers include bricklayers, carpenters, cement
masons, hod carriers, laborers, plasterers, tile setters, terrazzo workers,
ready-mixed concrete truck drivers, and other workers. Portland cement
products include concrete, mortar, plaster, grout, stucco, terrazzo, and
other products.
What Problems Does Cement Cause?
Four types of skin
problems happen most often among cement products workers:
- Dry skin or irritation (mild ICD)
- Irritant contact dermatitis (ICD)
- Allergic contact dermatitis (ACD)
- Caustic burns (alkaline burns)
Skin problems can be mild and short-lived or severe, persistent, and disabling. Problems can happen after single or multiple exposures. It is difficult, if not impossible, to predict who will get skin problems based on experience or on medical tests.
Dry
Skin or Irritation ( Mild ICD)
Dry skin or irritation
may include scaling, it chiness, burning, and redness.
Dry skin may also
be called xerosis. Portland cement exposure can lead directly to dry skin
or irritation.
Irritant
Contact Dermatitis (ICD)
Irritant contact
dermatitis (ICD) can be acute or chronic. Symptoms may include stinging,
pain, itching, blisters, rash, dead skin, scabs, scaling, fissures, redness,
swelling, bumps, and watery discharge. Sometimes irritated skin may become
infected. Exposure to portland cement can lead directly to ICD without
first causing dry skin.
Alkalinity is essential in the development of irritant contact dermatitis from portland cement. 3 Cement makes the skin’s barrier layer more alkaline and permeable. As the barrier layer becomes permeable, repeated contact with abrasive particles in cement products may contribute to ICD and ACD.
It can be difficult to recognize ICD by its appearance or morphology alone.4 Proper diagnosis of work-related ICD requires a complete work history and a physical examination.
 |
Irritant contact dermatitis (ICD) . Alkalinity is essential in the development of irritant contact dermatitis from cement. At alkaline pH, human skin is more permeable, repeated contact with abrasive materials may contribute to ICD and ACD. |
Allergic
Contact Dermatitis (ACD)
Allergic contact dermatitis (ACD) is an immune response. It is like other allergies but it involves the skin. ACD includes many of the same symptoms as ICD.
 Most
portland cement contains metals or other chemicals which are sensitizers,
or allergens. Foremost among them is hexavalent chromium (Cr
6+
) . Others may be present in admixtures: accelerators, water reducers,
superplasticizers, retardants, air entraining agents, or polymer-modified
systems.
Most
portland cement contains metals or other chemicals which are sensitizers,
or allergens. Foremost among them is hexavalent chromium (Cr
6+
) . Others may be present in admixtures: accelerators, water reducers,
superplasticizers, retardants, air entraining agents, or polymer-modified
systems.
Sensitivity to Cr 6+ and ACD may slowly develop in Portland cement products workers after many years of exposure to soluble chromium in cement. It is even possible to develop ACD up to five years after exposure to Portland cement has ended.5
ACD can develop without any warnings, such as local irritation. ACD is difficult to cure. The allergy may last a lifetime, with symptoms recurring after each exposure.
Caustic
Burns (Cement Burns)
Caustic burns
(cement burns) are chemical burns. Second or third degree burns may occur
after relatively short exposures to fresh mortar, concrete, grout , and
other Portland cement products. Cement burns look like other burns. They
produce blisters, dead or hardened skin, or black or green skin. Cement
burns can lead to allergic dermatitis. In addition, chromate sensitivity
can exacerbate the severity of cement burns.
The occurrence of alkaline burns from Portland cement is well documented. No official data exist on the annual number of cases. A statistically valid 1997 survey found cement burns among 35% of apprentice concrete masons nationwide.6
In severe cases, these burns may extend to the bone causing disfiguring scars, even disability. Some may require skin grafts.
Refer cement burns to a medical specialist without delay. When a worker feels a cement burn, much damage already has been done and further damage can develop unless medical treatment is received.
 |
Cement burns. The occurrence of alkaline burns from Portland cement is well documented. In severe cases, these burns may extend to the bone and cause disfiguring scars, even disability. |
Why
Worry About Portland Cement ?
Ted Jason' s problems are not uncommon. You probably know many workers with skin problems from cement. Portland cement is estimated to account for 25% or more of all work-related skin problems worldwide. 7
Reported lost work
days for skin problems in U.S. masonry trades are 2.5 times the national
average.8
Concrete workers
lose time at 7 times the national average. Concrete workers report 4 times
more lost work days for skin problems than do all construction workers.8
Some 5 to 15% of workers coming into contact with Portland cement that contains hexavalent chromium may suffer allergic contact dermatitis, a rate as high as 25 times that of the general population.9 This dermatitis may persist in 20 to 40% of workers without further exposures, even after they leave the trade.
Experts agree that reported lost time is just the small tip of a very large iceberg of skin disease. One indication of how prevalent skin problems are comes from a statistically valid survey of apprentice cement masons.
In 1997, 442 apprentices were surveyed using a questionnaire derived from one used by NIOSH.6 The response rat e was 100%. The mean age of t he surveyed apprentices was 27; the most frequent age was 20. The mean number of years in the industry was 3.3.
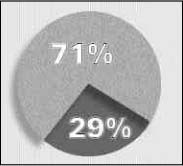 |
71% of apprentices had one or more skin problems. Only 29% reported no skin problems. |
A surprising 71%
of the apprentices reported one or more skin problems in the previous
12 months, including rashes, bumps, blisters, fissures, scaling, redness,
oozing, burning, and pain. Only 29% reported no skin problems.
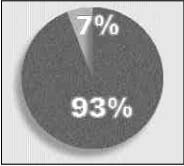 |
Only 7% of apprentices with skin problems reported lost time or physician visits for those problems. |
Only 7% of those reporting skin problems reported lost time or physician visits for their problems. 93% of the apprentices with skin problems continued to work without seeking medical treatment —setting themselves up for lifelong health problems. (Also see Halbert .9) Asked whether they had had ‘eczema’ or ‘ dermatitis’ at any time during their careers, only 3% of surveyed apprentices said yes, indicating possible lack of medical diagnosis.
Studies show poor
prognosis for complete clearing of occupational contact dermatitis, once
established. Recent studies show that 30-55% of patients have continued
problems with the skin disease at follup up. 10,11,12,34
Official reports of lost work days are not always reliable indicators
of the rates skin problems among Portland cement products workers. More
accurate estimates may come from statistically reliable surveys.
Skin has two primary
layers. Together, both are less than 1/ 8-inch thick.
- The epidermis ( outer layer) is only 1/ 250th of an inch thick.
- The dermis is only 1/50th to 3/25ths of an inch thick.
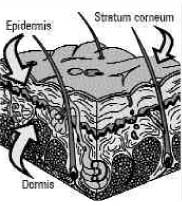
The dermis and epidermis contain oil glands, hair follicles, and sweat glands—all are like tiny channels through the skin letting in some foreign substances. Skin also contains blood vessels. Some chemicals can penetrate the skin and enter the bloodstream.
The layer of dead surface cells at the outer epidermis is the stratum corneum. Leading researchers now call it “ a biosensor that regulates the epidermal lipid and DNA-metabolic responses to a variety of insults.” 13 The stratum corneum is a "thin membrane of keratimized corneocytes in a 'brick and mortar' structure."14 It has the most mechanical strength of all the layers of the epidermis.4
The old model of skin disease assumed that skin responds directly to external insults. The response included conditions like inflammation, rashes, or even scar tissue.
Scientists can now detect skin function at the molecular level due to advances in bioengineering technologies.
The ‘ Signal Cascade’
The resulting new
model shows that external ‘insult’ triggers a ‘cascade
of molecular signals’ at the outer layer of the stratum corneum (‘permeability
barrier’) . This causes release of enzymes and formation of proteins
and ultimately may lead to the trapping of inflammatory disease-specific
cells in the dermis.13 The outcome is repair of the injured
barrier and/or symptoms of various skin disorders.15
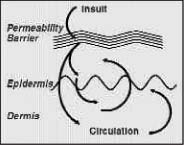 |
The skin is the single largest organ. It covers 20 square feet of surface. The skin's purpose is to protect the body from external substances, chemicals, and bacteria. The 'permeability barrier' plays a major role in maintaining healthy skin in the new outside-to-inside model of skin disease. |
So the ‘permeability barrier’ plays a critical role in maintenance of healthy skin.14 Any insult that disrupts the barrier injures the epidermis. Disruptions of the permeability barrier produce a response of recovery or repair. This may lead to normalization of barrier function within hours to days, depending on age and severity and persistence of the insult.13,15
When barrier disruption
is persistent , these processes become chronic. In some individuals, the
repair response compensates for insults and produces 'hardening.' Hardening
is a state of accommodation.
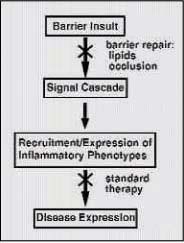 |
Normalization of the barrier function should be a standard part of treatment of skin problems. 13,15 Recovery or repair of the ‘permeability barrier' requires acidification of the stratum corneum as discussed in more detail in Chapter 4. |
Workers whose skin
has hardened may experience less irritation. However, epidermal hyperplasia
and inflammation persist , 15 leaving skin at risk of disease.
Others may never accommodate to irritants and never experience ‘hardening.'
“ ... [ M]aintenance of an acidic stratum corneum pH, either by preservation
of the lipid barrier or by exoneously applied acidic buffers, is important
to normal skin barrier function.” 15 The new model of
skin disease is the basis for these two main methods of preventing occupational
skin problems that are the focus of this guide:
- Preventing 'INSULT' means avoiding contact with irritants.
- Initiating Barrier Recovery requires extracellular acidic pH.15
The role of pH in barrier maintenance and repair is discussed further in Chapter 4.
What ‘Insults’
Initiate Skin Problems?
Skin may be affected
by one or more ‘ insults’:
- worksite materials,
- worksite conditions,
- environmental factors, and
- individual factors.
Worksite Materials
Worksite materials can start skin problems. Some materials insult and injure skin. Some also pass through it to the bloodstream.
Portland cement is very alkaline (caustic) when wet so it affects skin surface pH. The moisture in eyes, mucus, and sweaty skin can contribute water to dry cement, releasing its causticity. Portland cement is hygroscopic so it draws moisture from skin. Cement products are abrasive and physically damage the skin surface, making it a less effective barrier against chemicals. These factors allow cement to cause dry skin and irritant contact dermatitis.
Sensitizers in workplace materials may cause allergic responses in some workers. The reaction may be local or widespread. Sensitization is an immune response. The immune system fights a foreign substance. Usually, the material causes no change on first contact. Once a person is sensitized, small amounts trigger a strong reaction. Many people cannot tolerate any further exposure.
Possible sensitizers used by cement products workers include: hexavalent chromium (Cr6+) in cement, chemical admixtures in concrete, epoxies, additives in rubber gloves, and other trace metals in cement.
Hexavalent chromium (Cr6+) is rated as a strong to extreme sensitizer. It is an important cause of allergic contact dermatitis. Cement's alkalinity increases skin absorption of this soluble chromate. Some studies show that Cr6+ penetrates the skin and enters the bloodstream. 7 If skin is mechanically damaged (cuts, abrasions), it is feasible that Cr6+ and other allergens can penetrate it .
Worksite skin cleaners too often are caustic and abrasive. They may contain sensitizers like lanolin, limonene, or perfume and they may contain irritants like alcohol.
Worksite Conditions
Worksite conditions
can determine whether a worksite material will cause skin problems.
- How long does the worksite material contact the worker’s skin?
- How often does a worker use the worksite material?
- Is there mechanical trauma or abrasion of the skin (a break in the barrier)?
- Is the worksite material trapped or occluded to the skin by gloves, creams, lotions, pet roleum jelly, or barrier creams?
- Are there adequate hygiene facilities?
Environmental Factors
Environmental factors can cause skin problems directly or they can work with other factors to increase skin problems:
Heat causes sweating. Sweat can dissolve chemicals on the skin. Heat increases blood flow at the skin surface and this increases the absorption of materials into and through the skin.
Cold dries
the skin and causes microscopic cracks, sometimes known as ‘winter
eczema.’ Cold changes blood flow at the skin surface and leads
to loss of feeling.
Humidity increases sweating. High relative humidity (RH) keeps sweat from evaporating. A 1998 study showed that epidermal homeostasis and barrier repair following acute insult are better supported in a low humidity (RH<10%) environment rather than in high humidity (RH>80%). 17 Recent data suggest 40-60% RH is optimal.
Sun burns and damages skin. Sun can increase absorption of chemicals. Some chemicals react with sunlight to cause photosensitization and photoirritation. Sun exposure alone can also cause skin cancer.
 |
'Insults' to the permeability barrier of the skin of cement products workers include wet cement, hexavalent chromium, and harsh worksite cleaners. |
Individual Factors
Individual factors can affect workrelated skin problems. These include:
- preexisting dermatitis
- predisposition
- knowledge
- attitude
- personal/work practices
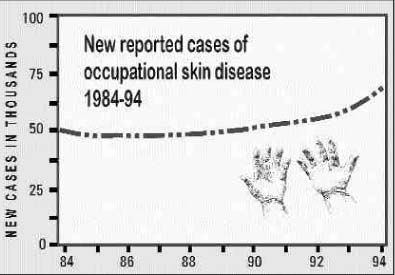
From 1983 to 1994, the rate of reported occupational skin diseases rose from 64 to 81 cases per 100,000 workers. In 1994, there were approximately 66,000 new reported cases of occupational skin diseases.
What Do Skin Problems
Cost ?
From 1983 to 1994, the rate of occupational skin diseases increased from 64 to 81 cases per 100,000 workers. In 1994, there were approximately 66,000 new reported cases of occupational skin diseases. Reported skin diseases are current ly about 10 to 15% of all work-related disease (BLS).
Moreover, occupational skin diseases are believed to be severely underreported. The true rate of new cases may be many fold higher than documented. No one knows how many family members are affected by contaminants brought home from the job.
Estimated total annual costs (including lost workdays and loss of productivity associated with occupational skin diseases) may reach $1 billion annually. Workers' compensation claims rates for occasional skin diseases vary by State and range from 12 to 108 per 100,000 workers per year. Self-reported occupational dermatitis prevalence in the 1988 National Health Interview Survey was nearly 2% (1,700 cases per 100,000 workers).
The costs to employers
include worker compensation disability claims, lower productivity, and
poor morale. The costs to the workers include reduced earnings, medical
bills, loss of a trade, social disability, embarrassment, and lower quality
of life.
The rates of most other occupational injuries and disease have fallen. But skin disease rates remain constant or actually increase. Little progress has been made, even though the causes are better understood and more methods of control exist now than ever before.
The NIOSH homepage (www.cdc.gov/niosh) presents additional information. Two reports explore the public health impact and epidemiology of contact dermatitis. 35,36
More than 92.7 million metric tons of portland cement were consumed in U.S. construction in one recent year, according to the Portland Cement Association.
The consumption of
Portland cement has increased every year since 1991.
 |
Brick setting (Photo courtesy of BAC) |
More than 1.3 million American workers in 30 occupations are regularly exposed to wet Portland cement products. Thousands more—such as ironworkers—are exposed to cement dust during the grinding of hardened cement products.
Cement is a mixture of lime, silicates, aluminum, iron, magnesium, and other additives such as gypsum, fly ash, and blast furnace slag. Portland cement is a component in:
- concrete—a mixture of Portland cement, water, fine and course aggregate, and chemical admixtures,
- mortar—a mixture of Portland cement, water, and fine aggregate,
- plaster—a mixture of lime, water, and sand, and may contain gypsum or port land cement as a binder ( Slaked lime or calcium hydroxide is extremely caustic.),
- Stucco—an exterior finish material composed of Portland cement, lime, sand, and water,
- terrazzo—an underlayer of Portland cement containing marble chips and tinted concrete,
- tile ground—a fluid mortar mixture consisting of Portland cement and water with or without aggregate, and
- other products
Portland Cement
Products Workers
More than 1,300,000
American workers in 30 occupations are regularly exposed to wet cement.
Their families may be exposed to cement dust on their work clothes.1
Following is a partial list of the construction trades workers who may be regularly exposed to cement:
 |
Concrete Finishing |
- bricklayer,
- carpenter,
- cement mason or concrete finisher,
- concrete truck driver,
- construction craft laborer,
- hod carrier,
- plasterer,
- terrazzo worker,
- tile setter, and
- others.
 |
Grinding cement underlayer for terrazzo (Photo courtesy of BAC). |
Portland Cement
Work Tasks
Below are some of the work tasks that expose construction workers to Portland cement:
- tending concrete pour,
- mixing and spreading grout ,
- preparing cement underlayer for terrazzo,
- hosing out ready mixed con, mixer, and chute,
- using mortar to set brick, cinder block, and other masonry,
- dismantling formwork contaminated by Portland cement,
- pouring, leveling, smoothing, and finishing concrete,
- attaching tiles to walls, floors, and ceilings,
- mixing mortar and providing it to other craftsworkers,
- mixing and applying plaster, stucco, and EIFS
- spraying Portland cement products such as fireproofing, gunite, or shotcrete,
- grinding of finished concrete, which releases cement dust.
 |
Setting tiles (Photo courtesy of BAC). |
The Nature of Cement
Cement has many properties which are damaging to skin. Cement is alkaline, or caustic. The pH of wet cement ranges from 12 to 13. Cement is hygroscopic, pulling moisture from the skin. Cement is abrasive. Cement may contain sensitizing chemicals and metals, such as hexavalent chromium (Cr6+)
 |
Applying stucco (Photo courtesy of OP&CMIA). |
The composition of cement varies somewhat from region to region. However, the alkaline, abrasive, and hygroscopic properties of cement in concrete, mortar, grout, plaster, stucco, and other products are universal.
Perhaps most frequently damaging of all these properties is the alkaline pH.
No matter what the cement product or work task, the most frequently damaging property of cement is its alkaline nature.
pH is a measure of
the acidity or alkalinity of a substance. The pH scale ranges from pH
0 on the acidic end to pH 14 on the alkaline end.
The acidic pH range
is pH <1 t o 6.9. the alkaline (base) ph 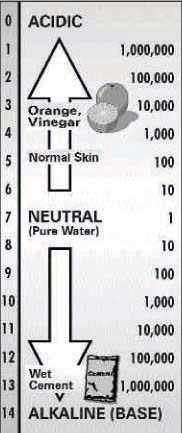 range
is pH 7.1 t o 14. Strong acids are pH 1 to 3. Strong alkalies (bases)
are pH 12 to 14.
range
is pH 7.1 t o 14. Strong acids are pH 1 to 3. Strong alkalies (bases)
are pH 12 to 14.
pH stands for “potential of hydrogen.” It refers to the concentration and activity of hydrogen ions in a substance in aqueous solution (water). Acids ionize in water to give H + (hydrogen) ions. Alkalies (bases) produce OH - (hydroxyl group) ions in water.
An ion is an atom
that has lost or gained one or more electrons and has acquired an electric
charge. Cement contains calcium hydroxide which liberates hydroxylions.
The use of scientific notations to describe the hydrogen ion concentrations of substances is cumbersome. So chemists began using the pH scale in 1909.
pH-neutral is 7. This is the pH of pure or distilled water. It is virtually free of hydrogen ions.
The pH scale is like the Richter scale for earthquakes. Both are logarithmic. On a logarithmic scale, the intervals between the numbers are not equal. Every whole number on the pH scale represents a 10-fold change in alkalinity or acidity.
pH 13 is one million times more alkaline than pure water at pH 7. pH is one million times more acidic than pure water.
Wet cement is extremely alkaline, with a pH value of 12 t o 13. Strongly alkaline material is caustic and corrosive to skin, eyes, and mucous membranes.
Wet cement is 10 million to one billion times more alkaline than normal human skin.
A recent study found that barrier recovery proceeds normally when exposed skin is treated with solutions buffered to an acidic pH. In contrast, the initiation of barrier recovery is slowed when exposed skin is treated with neutral or alkaline pH solutions, regardless of buffer composition.15
The pH of Normal Skin
Normal skin is pH 4.5 to 5.5, meaning it is moderately acidic. The acidic pH of skin has been recognized for a century. However, the function of the ‘acid mantle’ of skin remains incompletely understood. Scientists believe it has to do with provision of the proper milieu for the extracellular processing of certain lipids (fats) required for barrier function. 4,13

Like an orange, normal skin is mildly acidic.
Contact with wet cement changes skin pH from acidic to alkaline. At alkaline pH, barrier recovery is slowed, damage is prolonged, and skin problems are exacerbated.15 Alkalinity is essential in the development of irritant contact dermatitis (ICD) from cement. 3
Alkaline pH contributes greatly to skin absorption of the hexavalent chromium (Cr6+) in cement.18 So absorption of Cr6+ may be increased when it contacts skin in cement.
Measuring pH
As a safety & health practitioner, you can measure the surface skin pH of cement products workers. Elevated pH is an indicator of portland cement residue on the skin.19 It demonstrates the effectiveness or ineffectiveness of protective measures. pH also serves as a feedback mechanism for education workers about the need to protect their skin from cement.
The best way to measure surface skin pH is with pH indicators, also known as pH color test strips. As an educational tool, pH test strips also can be used to measure the pH of cement residue on car seats, steering wheels, boots, glove interiors, and more.
Full range color test strips (pH 1 to 14) work best for cement contamination.
How To Use A pH
Test Strip
To test skin or dry surfaces, moisten a strip in distilled water. Apply it to the test surface. To test a liquid, dip the test strip in the liquid.
The strips come with a color coded scale. Hold the test strip next to the scale. Hold the test strip next to the scale and wait for it to change color. Then match it with the color on the scale to find the pH value.
pH represents the acidity or alkalinity of a watery solution on a scale. Pure water has a pH of 7. pH 7 is considered pH-neutral. Citrus and vinegar are pH 3.5—10 times more acidic than normal skin. Wet cement is 10 million to one billion times more alkaline than normal skin.
 |
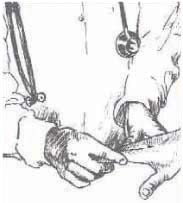
One of the authors tests the surface skin pH of a cement products workers during the first evaluation of buffering solution. Even though this worker wore gloves, his skin surface tested at pH 11. (Normal skin is pH 4.5 to 5.5) In the absence of proper hygiene, a residue of wet cement had contaminated the insides of his gloves and his hands |
pH Testing Exercises
Supplies: dry Portland cement, household vinegar, one gallon distilled water, pH test strips, plastic glasses, plastic spoons, bar soap, liquid soap. Along with vinegar, you may consider testing one of the buffering or neutralizing products.
- Dip a pH strip in distilled water. Compare the strip with the color key. What does it tell you about the pH of the water?
- Add a little portland cement to the water and stir. Dip a new pH strip into the solution. Compare it to the color key. What happened to the pH?
- Add a little vinegar to the cement water and stir. Dip a new pH strip in the water. What happens? What is the pH now? What does it mean?
- Dip a new pH strip in a clean glass of distilled water. Lay the strip on the surface of the bar soap. What is the pH of the bar soap? What does it mean?
- Take a new pH strip and pump some liquid soap on it. What is the pH of the liquid soap? What does it mean?
 You
also can test the pH of exposed hands, gloves, hard hats, or the seats
and steering wheels in cars or trucks. Just dip a pH strip in distilled
water and lay it on the surface to be tested.
You
also can test the pH of exposed hands, gloves, hard hats, or the seats
and steering wheels in cars or trucks. Just dip a pH strip in distilled
water and lay it on the surface to be tested.
A pH test meter can be used to test tool rinse bucket pH. But cement particles in the water may clog this instrument.
pH Testing Conclusions
Cement product s workers probably will find the alkaline residue of wet portland cement on their skin and even on their clothes, their boots, their vehicle interiors, and elsewhere.
Removing t his alkaline cement residue requires clean running water and pH-neutral 20 or acidic soap. It may be protective to use a buffering solution in the workplace to normalize the pH of surface skin.21,22
Wearing gloves without
good hygiene appears to be no more productive than wearing no gloves at
all.3,19 and in fact may be worse.
 |
Removing alkaline wet cement residue requires clean running wash water and pH-neutral or slightly acidic soap. Use of a buffering or neutralizing solution to normalize surface skin pH may be protective. Wearing gloves without good hygiene facilities and practices appears to be no more protective than no gloves at all. 3,19 |
More About Acids and Alkalies
Acids and alkalies (bases) react with one another so that the properties of both are lost to form water and a salt. The result is a more pH-neutral solution.
![]()
So adding an acid to an alkali tends to neutralize its pH. For example, adding vinegar to cement water can reduce the pH. But it also may generate heat.
Buffers are another choice for controlling surface skin pH. If added to an alkali, a buffer may reduce pH without generating heat.
Treating Skin with Solutions Buffered To An Acidic pH
Buffering solutions are equilibrium systems that maintain a constant pH when combined with acids or alkalies. A buffer can neutralize either an acid or an alkali. Buffering solutions typically contain similar amounts of a weak acid and a salt of its conjugate base.
Compared with acids, buffers generate less heat and can maintain the desired pH over a longer period of time. Phosphates are often used as buffering agents.
One important study of the role of pH in skin barrier repair following external insult concluded that "...maintenance of an acidic stratum corneum pH, either by preservation of the lipid barrier or by exoneously applied acidic buffers, is important to normal skin barrier function. [emphasis added]".15
Portland cement products workers may have difficulty in preventing 'insult' from wet cement. When cement residue accumulates on the skin, the application of a buffering solution may be beneficial in restoring the acidic pH of the stratum corneum, thus permitting the initiation of barrier repair and preventing skin problems.
A recent evaluation of buffering solution found that concrete truck drivers using a pH 5.5 buffering solution were more likely to see improvements in their skin problems than were drivers who used other treatment methods during a 30-day period.22
Commercial product s are marketed for acidifying t he skin’s stratum corneum. Neutralitetm is a pH 5.5 buffering solution. Mason's Hand Rinsetm is an acidic rinse. In theory, either product or similar products can be helpful if they normalize surface skin pH.
In addition to reducing the corrosive effect of cement, normalizing pH through the application of a buffering solution may convert hexavalent chromium (Cr6+) to trivalent (Cr3+). This would decrease skin absorption of Cr6+, reducing the risk of ACD.
| A Partial List of pH-Neutral or Moderately Acidic Soaps |
| Liquid Soaps |
| Aloe Vera 80 |
| Cetaphil |
| Dial |
| Dove |
| Gillette Wash |
| Ivory |
| Jergens |
| Lever 2000 |
| Neutrogena |
| Noxema |
| pHisoderm |
| Softsoap |
| Bar Soaps |
| Caress |
| Dove |
| Oil of Olay |
This soap list is advisory only . To obtain reliable information, ask the soap's manufacturer for an MSDS. A pharmacist can recommend pH-neutral or moderaltey acidic soaps.
Industry leaders
often ask whether cement can be modified to reduce the skin hazards. Different
modifications are proposed depending on the specific skin problem.
Remember, cement
causes two main problems: irritant contact dermatitis (ICD) and allergic
contact dermatitis (ACD). Cement causes ICD because it is alkaline, hygroscopic,
and abrasive. Cement causes ACD because it contains sensitizers, not ably
hexavalent chromium (Cr6+).
Worldwide, there
have been several experiences with modifying cement to prevent allergic
contact dermatitis (ACD) from hexavalent chromium. Before reviewing results,
let’s examine the cement manufacturing process.
In the hierarchy of hazard controls, the best and most effective measure
is always substitution of a less hazardous chemical. Product modification
is a type of substitution. If product modification is feasible, it can
often reduce or eliminate the need for other hazard controls.
Cement Manufacturing
Most cement manufacturing plants are located near quarries. Quarries mine the raw materials needed to make cement .
Huge quarried boulders of stone such as limestone and shale are dumped into an impact crusher. These raw ingredients, along with small amount s of iron ore and clay, may then be fed to a grinding mill where steel balls tumble to pulverize the material into a powder.
This powder may then be loaded into giant steel rotary kilns. The typical kiln may be about 200 feet long and 15 feet in diameter. The kiln interior is lined with refractory brick. As the kiln rotates, the inside temperature reaches 3,000 to 4,000 degrees Fahrenheit. The solid material must reach 2,600 degrees Fahrenheit.
The heat causes a chemical reaction in the raw materials as they slowly transform into portland cement. At this point in the process the cement compound is called clinker.
Clinker is dark gray chunks like volcanic rocks. The fully processed clinker falls out of the rotary kiln and down into t he clinker cooler where it cools it off for reprocessing.
The clinker is then ground in a giant rolling tube called a ball mill. Gypsum is added during t his grinding process.
The ball mill is filled with several tons of metal balls. Often, these balls are chrome or chromeplated. As the mill spins, the metal balls crush the clinker into an extremely fine dust and mix it with the gypsum until it becomes portland cement.
Samples of the finished product are taken to a lab for strength and consistency testing. The final product is shipped in bulk by truck and rail or packaged in bags. Cement is used in the manufacture of plaster, stucco, mortar, grout, and other cement products.

The major sources of chromium in cement are the kiln feed raw materials, refractory brick in the kiln, and wear metal from the media and liners and in the mills.5

The chromium content of Portland cement may range between 1 and 30 ppm but is usually less than 20 PPM The hexavalent chromium (Cr6+) content is usually less than 30% of t he total chromium. When clinker is ground wit h chrome alloy balls, t he Cr6+ content of the cement may increase to more than twice that present in the original clinker.5
The European Experience: Reductions in Chrome-Induced Dermatitis
Recognition of the connection between hexavalent chromium in portland cement and allergic contact dermatitis in cement products workers first emerged in Europe during t he 1950s. As the evidence mounted, some European countries acted to limit exposure to hexavalent chromium in cement products.
By law, Denmark and Sweden require cement manufactures to produce cement whose concentrations of Cr6+ are 2ppm or less. In these countries, a patented process is used which involves intergrinding of clinker, gypsum, and ferrous sulfate heptahydrate to reduce chemically the Cr6+ to trivalent chromium (Cr3+).
Cr3+ is not harmful to human skin because it is not absorbed by the skin.
A similar patent was granted to an East German company in 1985 and another to a Japanese firm in 1991. Additional patents were granted in other countries in subequent years.
Finnish, Danish, Swedish, and other scientists have published studies showing that this method of modifying portland cement at the plant has greatly reduced ACD in Portland cement products workers in Scandinavia and Singapore.18,23,24,25,26,38 ICD rates in these countries remain unchanged.
ACD from portland
cement is a common occupat ional dermatitis among construction workers
and a reduction in the chromate content of cement would be a reasonable
preventive measure.18,27
Reductions of hexavalent chromium in portland cement, required by law
in Europe and Singapore, have produced reductions in the rates of allergic
contact dermatitis (ACD) in those counties
The American Experience:
‘More Study Is Needed’
In response to California’s Proposition 65 regulations, some American cement manufacturers experimented with iron sulfate in an effort to reduce Cr6+ in Portland cement .
In a published report of the results5 and in other forums, several reasons have been given for the failure to replicate the Scandinavian results.
"...[I]t would seem quite difficult to successfully intergrind ferrous sulfate heptahydrate with clinker and gypsum in any large finish mill due to the large circulating load of the mill/separator system, the elevated mill temperatures, and the high-volume air sweep. All of these factors would lead to the ready oxidation of ferrous iron."5
More than 120 plants make U.S. cement and t he product ships long distances in this country. If ferrous sulfate is added, the time it takes to transport the cement may result in spontaneous oxidation of the ferrous ion to the ferric form, rendering the ferrous sulfate inactive.
The addition of ferrous sulfate during grinding is a patented process. Royalties and the cost of the ferrous sulfate (variously estimated at $.05 to $1.00 perton) would increase the cost of American portland cement products. Added costs may be incurred in reconfiguring manufacturing processes to allow for the addition of ferrous sulfate.
As an alternative, some researchers have recommended that ferrous sulfate be added during mixing of concrete or when delivering premixed cement products to the worksite. 9,24
Finally cement products may be modified in another way to reduce Cr6+ levels. Slag can be substituted for clinker at the plant. 25

American manufacturers express concern about possible effects of such methods on the structural integrity of finished concrete. For example, some argue that addition of substantial amounts off errous sulfate to concrete might cause durability problems or necessitate adjustment of the amount of gypsum added.
Concrete in Europe and Singapore appears unaffected by modifications to cement in those countries. Manufacturers point out that American specifications for concrete are rigid, that any changes must be well researched, and that research is in fact ongoing. So change may be possible some day.

One difference between American and European cement manufacturers is the
distances between the plants and the points of consumption. American cement
is transported greater distances.
Neutralize pH at the Plant?
Some in the industry have asked manufacturers to reduce the alkalinity of cement.
By nature, wet port land cement is pH 12 to 14. Attempts to neutralize the pH of cement would chemically alter it . For example, the amount of buffering solution needed to neutralize a batch of cement at the plant would overwhelm the chemical formulation of the cement . It would no longer be cement.
Rather than attempt to neutralize the pH of an entire batch of cement at the plant, it seems more feasible to reduce the pH of the comparatively small amount of cement that may contact the surface skin of cement products workers at the jobsite. This can be done with a neutralizing or buffering solution.
As an additional benefit, neutralization of pH also may convert Cr6+ t o Cr3+, rendering the iron sulfate controversy irrelevant.
Neutralizing the pH of portland cement during the manufacturing process is not feasible.
Protecting skin is not simply a matter of wearing gloves. A substantial portion of cement products workers already wear gloves. To be effective, glove wear must go hand-in-hand with proper hygiene. Hygienic practices and use of the correct gloves will prevent contact with cement. Glove wear without good hygiene is no more protective than no gloves at all.3,19 In fact, it can make problems worse.
This chapter presents
the best protective practices for preventing skin problems from Portland
cement :
- Best practices
at home.
- Best practices
at work.
- Best practices in emergencies.
Not everyone can do all these practices. But every cement products worker should do as many as possible, beginning with the easiest ones. There is no guarantee that any or all of these practices will prevent skin problems from Portland cement . But these practices are recommended by experts and they represent the best protections known.
Best Protective
Practices at Home
Best protective practices are recommended by experts based on results
of scientific studies and field experience. A Printer ready worker safety
pamphlet explaining best practices to cement products workers, is available
towards the end of the document.
pH-NEUTRAL OR ACIDIC SOAPS
 Portland
cement products workers should wash with pH-neutral or moderately acidic
soaps.
Portland
cement products workers should wash with pH-neutral or moderately acidic
soaps.
Alkaline soaps may be fine for the general population. But cement products workers who wash with alkaline soaps continue to 'insult' their skin with alkalies. Remember, alkaline pH impedes barrier repair.15
If cement products workers wash with pH-neutral or acidic soaps, it may help restore the desired pH balance of the surface skin.
WASH WORK CLOTHES
SEPARATELY
Warn cement workers to launder work clothes separately to protect family or roommates. Run washer empty after work clothes load.
Remember Ted Jason's daughter?
Construction workers
are motivated to take protective measures when they believe they are protecting
their children.
2
So convincing portland cement products workers to launder work clothes
separately may be a good first step to adopting more best practices.
Best Protective
Practices at Work
A WORKER NEEDS 5 TO 7 GALLONS OF CLEAN RUNNING WATER PER DAY
 Workers
need clean water for washing before work, whenever they break, and at
the end of the shift. Water can be brought to the jobsite in tanks on
wheels. Many employers would be surprised at how economical it can be
to provide decent hygiene for workers. They might also be surprised at
the improved morale and productivity that result.
Workers
need clean water for washing before work, whenever they break, and at
the end of the shift. Water can be brought to the jobsite in tanks on
wheels. Many employers would be surprised at how economical it can be
to provide decent hygiene for workers. They might also be surprised at
the improved morale and productivity that result.
Consider providing buffering spray to reduce the pH of contaminated surface skin.
Prohibit cleaning
with abrasive or solvent-containing products. These include waterless
handcleaners like alcohol-based gels or or citrus cleaners based on limonene.
Such cleaners are not suitable for cement exposure.
Removing alkaline wet cement residue from skin requires clean running
wash water and pH-neutral or slightly acidic soap. It may be helpful to
use a buffering or neutralizing solution to normalize surface skin pH.
PROMOTE HAND WASHING
BEFORE PUTTING ON GLOVES AND AGAIN IF GLOVES ARE REMOVED
Gloves on dirty hands trap contaminants against the skin. Workers should wash with pH-neutral or slightly acidic soap and clean running water, as noted in the Portland Cement Association's sample MSDS. If workers remove gloves during work, they must wash again. If not, cement will enter gloves. Workers should not rinse their hands in tool rinse buckets.
 ENCOURAGE
HAND DRYING
ENCOURAGE
HAND DRYING
A worker should dry hands with a clean cloth or paper towel before putting on gloves.
DISCOURAGE LEAVING
CEMENT ON SKIN OR CLOTHES
When wet cement gets on permeable clothing, remove it immediately. When wet cement gets on skin, wash with clean water and pH-neutral or acidic soap. At the least, consider using a buffering spray to reduce alkalinity.
ENCOURAGE LONG SLEEVES TAPED INSIDE GLOVES
Many experts recommend wearing long sleeve shirts taped inside gloves.
 DISCOURAGE
JEWELRY AT WORK
DISCOURAGE
JEWELRY AT WORK
Cement can collect under rings, watches, or necklaces. Wet cement trapped against skin for long periods of time is hazardous.
ENCOURAGE WORKERS
TO CHANGE WORK CLOTHES AT WORK
 Removing
work clothes at work cuts exposure for workers and their family members.
It keeps cement out of the car or truck interior.
Removing
work clothes at work cuts exposure for workers and their family members.
It keeps cement out of the car or truck interior.
If work clothes cannot
be left at the job, they should be taken home in a separate container.
A trash bag works great.
DISCOURAGE USE OF LANOLIN, PETROLEUM JELLY, AND OTHER SKIN SOFTENING PRODUCTS AT WORK
Skin-softening substances can seal or occlude portland cement residue to skin, can increase the skin's ability to absorb contaminants, and can irritate and sensitize the skin.
Never use petroleum jelly or other emollients to treat cement burns. Applying such products can intensify burns by trapping the cement residue against the skin.
 Skin-softening
products should be applied only to clean skin in clean environments. A
cement products worker may use these products, if desired, at home after
showering or bathing with pH-neutral or slightly acidic soap. A recent
study found one common product effective in skin barrier enhancement.28
Skin-softening
products should be applied only to clean skin in clean environments. A
cement products worker may use these products, if desired, at home after
showering or bathing with pH-neutral or slightly acidic soap. A recent
study found one common product effective in skin barrier enhancement.28
Some skin-softening products may contain fragrances, lanolin, or other chemicals that can cause ACD in susceptible workers.

 DISCOURAGE
BARRIER CREAM USE
DISCOURAGE
BARRIER CREAM USE
Barrier creams or 'invisible gloves' are not recommended for Portland cement work. 29,39 The abrasive cement probably breaks the seal of the barrier cream. Also, reapplying the cream in the work area may occlude the seal cement to the skin.
SELECT PROPER
GLOVES
Consult a glove manufacturer to select the right glove for the hazard.
Manufacturers often recommend butyl gloves or nitrile gloves for caustics
like cement. Cotton or leather gloves may become saturated with wet cement.
Cotton gloves dipped in butyl rubber or similar materials to coat the
fingers, knuckles, and palms may provide adequate protection. Make sure
gloves fit. Loose gloves let cement in.
ENCOURAGE GLOVE LINER USE
Glove liners of thin cotton help make gloves more comfortable. They can help keep hands clean and dry. But they must not be contaminated with cement inside the gloves. The goal is to keep the insides of the gloves clean.
ENCOURAGE DAILY
CLEANING
Clean reusable gloves daily. Follow t he manufacturer’s instructions. Place clean gloves in a baggie. Store gloves away from tools and materials in a dark, dry place where the temperature is not too high.
THROW OUT GROSSLY
CONTAMINATED GLOVES
Sometimes gloves get so contaminated they cannot be cleaned. Throw them out.
 PROMOTE
DISPOSABLE GLOVES
PROMOTE
DISPOSABLE GLOVES
Disposable gloves can make it easier to keep hands clean. Disposable gloves can be less expensive than reusable gloves. The only drawback to disposable gloves is that workers sometimes wear them too long. To remove disposable gloves, peel back from the top, turning them inside out. Discard disposable gloves at the jobsite each day.
Disposable gloves can make it easier for workers to keep their hands clean. Disposable gloves can be less expensive than reusable gloves. The draw back to disposable gloves is that workers often wear them too long.
How To Choose
Gloves
The experience of workers in using personal protective equipment (PPE)
to provide a barrier between wet cement and their skin has produced mixed
results. At least one study found the same rates of skin disease among
workers wearing and not wearing gloves.3
The main goals for
successful glove wear are:
- keep materials
from penetrating or saturating gloves
- keep glove insides clean and dry
- gloves fit
- gloves are cleaned
daily
- gloves are discarded
when worn out or grossly contaminated
- gloves are correct for worksite materials
- impermeable rubber
or butyl nitrile
- cotton with digits/palms
dipped in butyl/rubber
- leather
Some gloves combine rubber or butyl with cotton, other fabrics, or leather. Glove thickness and the length of the cuffs vary by task or worker preference. All-fabric or leather gloves are not recommended because they may become saturated with wet cement.
Gloves on workers are no proof of protection. Don't fool yourself: Without good hygiene, gloves are no better than no protection at all.3,19 If workers can't wash with clean running water and pH-neutral or acidic soap whenever they remove their gloves, the insides too easily become contaminated.
Potential problems
to consider when selecting gloves include: Workers should be
allowed to choose among equally protective gloves, whenever possible. Below are the
websites of two well-known glove manufacturers. Gloves can be purchased
from these and others or through a local safety supply store listed in
the business section of the telephone directory.

http://www.bestglove.com
http://www.ansell-edmont.com
Consider using pH strips regularly to test the pH inside of workers'
gloves as a way of monitoring the effectiveness of protection
SHOW WORKERS HOW
TO REMOVE REUSABLE GLOVES
When workers wear the correct gloves, they still must avoid contamination when they remove the gloves. As a safety & health practitioner, you can demonstrate proper met hods for cleaning, removing, and storing gloves. Before removing gloves, clean the outsides by rinsing or wiping off wet cement. Follow manufacturer's instructions. Watch for pinholes which can let in contaminated rinse water.

To remove gloves,
loosen them on both hands. Hold hands down so contaminated water will
not drip onto skin or clothing.

Remove the first glove only to the fingers. The cuff of the glove will remain over the palm.

Now, grabbing the
second glove with the first glove, remove the second glove. The first
glove should slip off.

Try to handle gloves
by the insides only. Don't touch the outsides.

URGE WORKERS TO
SEE A PHYSICIAN FOR SKIN PROBLEMS
Any worker with a
persistent skin problem, even a minor one, should see a physician. A statistically
valid survey of apprentice cement masons showed only 7% of those with
skin problems saw physicians even though 71% had had problems in the last
year.6 Some did not think the problems were serious. Others were afraid
of losing employment.
To get effective treatment , the cement products worker must inform the physician about products used at work. The goal is to provide medical treatment for a health problem.
A Physician Alert brochure is available from CPWR – Center for Construction Research and Training (301-578-8500 or www.cpwr.com) . The brochure can be given by a worker to a doctor, along with the product Material Safety Data Sheet.
Encourage workers
to follow the physician's prescriptions and recommendations. That action,
combined with other best practices, can lead to the successful control
of most cement-related skin problems.
A worker should see a physician for any persistent skin problem, no matter
how minor. In the case of allergic contact dermatitis, early diagnosis
and treatment can make the difference between controlling the problem
and suffering lifelong disease.30
 REVIEW
THE MODEL MSDS
REVIEW
THE MODEL MSDS
Find the best Material
Safety Data Sheet in the industry and review its recommendations.
The best MSDS is
the one that is most complete and provides the most protective recommendations.
The Portland Cement Association ( PCA) has published a sample MSDS report.20
The sample MSDS also addresses the respiratory hazards of portland cement
. 40
Remember, this MSDS is only the minimum guideline. With a little creative thought and not too much effort, employers and workers can do a lot more to prevent skin problems.
Best Practices in Emergencies
Dusty clothing or clothing wet with Portland cement fluids should be removed promptly and laundered separately before reuse.
Workers must wash wet cement from the skin with clean water and pH-neutral or acidic soap. Workers cannot rely on pain or discomfort to alert them to skin damage.

CEMENT BURNS
An acid will burn skin immediately. Cement is sneakier. A worker can work with wet cement on the skin for hours without feeling any discomfort . But the alkaline burns of the port land cement are damaging the skin microscopically. That damage may be just a cement burn or it also may be the cumulative injury that leads to irritant or allergic dermatitis.
Cement burns are alkaline burns (caustic burns). Cement burns progress. This means they get worse even without more exposure. Anyone who feels a cement burn starting should go immediately for emergency treatment in an ER or by a burn specialist. Don't assume the burn will not get worse. By the time an employee becomes aware of the burn, much damage has already been done and further damage is difficult to stop.
Medical experts recommend flushing the skin with lots of clean water. Some suggest adding vinegar, citrus, or a buffer to the water to neutralize the caustic effect . 15,21,31,32,33,37
When cement burns are treated medically, recovery takes place within two to three weeks. If untreated, these burns take much longer to heal, if they ever do.
Almost everyone agrees the construction industry must do more to protect workers from skin problems. As a safety & health practitioner, what resources can you use to improve protection for cement products workers?
The PRINTER-READY
PULL OUTS in this guide can help: Worker Safety Pamphlet, Best
Practices Checklist, and Symptoms Questionnaire. This chapter also
presents some additional tools and pointers to help you achieve your goals.
Save Your Skin Booklet
Save Your Skin, an 8-page booklet explaining proper glove wear f or work with wet Portland cement products. (Remember, 'wet cement' can include cement dust on moist skin.)
CPWR – Center for Construction Research and Training
301-578-8500
www.cpwr.com
Sample Material Safety Data Sheet
The Portland Cement Association offers a sample Material Safety Data Sheet. 20 Recommendations include washing on the job with running water and pH-neutral soap.
Portland Cement Association
847-966-6200
Training Video for Concrete Work
Skin Safety with Cement and Concrete, a worker training video, is for sale from the Portland Cement Association. The video presents safety tips and hazard information. It focuses on cement burns rather than on preventing dermatitis.
Portland Cement
Association
Video Sales: 1-800-868-6733
Cement Burn Kit
The Cement Burn Awareness Kit is available for purchase from the National Ready Mixed Concrete Association for use in educating Portland cement products workers.
The kit contains color photographs of severe cement burns, warning tools, and a sample MSDS to help prevent cement exposure.
National Ready
Mixed Concrete Association
900 Spring Street
Silver Spring, MD 20910
1-888-84-NRMCA
FAX 30l-585-4219
Save Your Skin Tool Box Pamphlet
Save Your Skin: 15-Minute Tool Box Session is an 8-page booklet explaining symptoms, skin problems, pH testing, and protective practices for work with cement products.
CPWR – Center for Construction Research and Training
301-578-8500 www.cpwr.com
pH Color Test
Strips
pH test strips (indicators) can be ordered from your local safety store
or direct from Markson LabSales, Inc., at 1-800-528-5114 or from Lab Safety
Supply at 1-800-356-0783. Prices vary somewhat . The strips seem expensive
but they are valuable tools for evaluation and education. Full range strips
(pH 1 to 14) work best for cement. pH strips permit reasonably accurate
measurement of pH on skin and other surfaces. See instructions for use
on
Buffers And Neutralizers
Commercial products are now marketed for buffering or neutralizing the pH of cement residue. NeutraliteTM; is a buffering solution. Mason’s Hand Rinseä is an acidic rinse. Each is spray-applied. In theory, these or similar products can be useful if they neutralize or buffer alkaline residue on the skin surface.
Neutralite Safety
SolutionTM
Force Field Technologies
P.O. Box 5381
Granbury, TX 76049
800-850-3908 FAX 817-326-5304
Mason's Hand Rinse
TM
Libby Laboratories, Inc.
1700 Sixth Street
Berkeley, CA 94710
510-527-5400 FAX 527-8687
Let's say you want to invest time and effort in improving conditions with the aim of preventing skin problems from portland cement.
How will you know if your efforts pay off?
You might say, “It's easy—I'll see the improvement with my own eyes. It will be plain to everyone.” But that may not be true.
Whether your responsibilities as safety & health practitioner involve five cement products workers or 500, you can set up a system for measuring t he success of your prevention efforts. This chapter gives some simple ideas about how to do it
There are two very good reasons to evaluate your prevention efforts. One is to get the feedback you need to improve your efforts. The other is to justify their continuation.
Compared To What ?
When you evaluate anything, you need a basis for comparison. Two classic methods of evaluation are ‘criteria-based' and ‘norm-based' comparison.
Criteria-based means comparing something with an objective standard that's set up ahead of time. For example, if a teacher grades tests by an objective standard and gives an ‘A' only for 100%, that's ‘ criteria-based' evaluation.
Norm-based means comparing something with other things in the same category. For example, if a teacher "grades on a curve" by comparing a student with other students in the class, that's 'norm-based' evaluation.
To measure your success in reducing skin problems from cement, first choose your own basis for comparison. Do you want to compare your results with an objective standard of 100% healthy skin and perfect protective practices? Or should you measure progress by comparing results with existing conditions?
Always remember that you are not evaluating the workers. You are evaluating the effectiveness of your own efforts to change their protective practices and to improve the protections provided by the employer.
Measuring Tools
Whatever comparison
standard you choose, here are three tools you can use to measure your
results. You might also think of other tools.
- Best Practices Checklist
- Skin Symptoms Questionnaire
- pH test s of
surface skin
Norm-Based Evaluation
Consider comparing the workers, as a group, with themselves before and after beginning your prevention efforts.
Before you begin, take some baseline measurements. You can use the Best Practices Checklist and the Symptoms Questionnaire in this guide. For example, watch workers on the job and take reports of what they do at work and at home. You are not comparing individuals. You are comparing the workers as a group before and after your efforts.
Which best practices are the workers currently doing? Which are they failing to do? Keep a written record of your observations. Have the workers complete the symptoms questionnaire. Assure them the information will not be released in personally identifiable form and that their answers will have no effect on their employment. Ask them to do a pH test of surface skin. Again, this is not a test of the individual worker. Instead it is a measure of the success of the protections implemented by you, the safety & health practitioner.
Once you have a baseline record, begin your effort to reduce skin problems. Teach workers best protective practices and make what improvements you can in working conditions.
When you think your efforts may be starting to pay off, repeat your measurements. If you made worksite observations, make them again. If you collected best practices checklists, collect them again. If you collected symptoms questionnaires, collect them again.
Now count the results and compare the ‘BEFORE' and the ‘AFTER.' If you or someone in your organization knows how to use a statistical software program, it can help your evaluation. Or you can count by hand calculator and determine where it appears there has been progress. Repeat the measurements again in a few weeks or a few months. Keep a long-term record of the outcomes.
Take the same measurements
periodically to assess progress. The results can help you adjust your
efforts.
Always remember that you are not evaluating the workers. You are evaluating
the effectiveness of your own efforts to change their protective
practices and to improve the protections provided by the employer.
What If Workers Are Transient?
In construction, workers often come and go. Turnover varies from company to company. Some larger companies have a steady cadre of core workers and hire or layoff more as projects demand. Other companies have no steady workers, only transient ones. This makes evaluation more difficult. But not impossible.
Always keep in mind that you are not evaluating individual workers. You are evaluating the success of your efforts by looking at all the workers as a group.
If all the workers are transient, you may not see immediate improvements in the symptoms checklist. But you should see improvements in the pH tests of surface skin and in compliance with best protective practices. This should help prevent future dermatitis.
Work With Others
By working with other organizations, you can help to reduce skin problems among the cement products workers whose safety and health is your professional concern. If possible, involve the health & welfare plan and implement a plan-wide evaluation in medical costs and workers compensation disability.
|
How
To Use The WORKER
SAFETY PAMPHLET. BEST PRACTICES CHECKLIST. Following the pamphlet is the Best Practices Checklist. Again, you can paste your organization’s name or logo in the box before copying. You can use the checklist to evaluate your efforts, to help workers remember the practices, and in other ways. SYMPTOMS QUESTIONNAIRE. You or a physician may find the questionnaire helpful in evaluating workers' skin problems. Anyone is free to reproduce any material in this guide for any purpose. |
INSTRUCTIONS: Place a checkmark on the line next to each
protective practice followed.
Best Practices Checklist
| BEST PROTECTIVE PRACTICES AT HOME | |
| ___ | 1. Use pH-neutral or acidic soap at home. |
| ___ | 2. Launder work clothes separately. |
| BEST PROTECTIVE PRACTICES AT WORK | |
| ___ | 1. Wash with clean running water and pH-neutral or mildly acidic soap. |
| ___ | 2. Wear correct gloves. |
| ___ | 3. Wash and dry hands before putting on gloves. |
| ___ | 4. Wash again whenever gloves are removed. |
| ___ | 5. Try using a neutralizing or buffering spray. |
| ___ | 6. Use disposable gloves or clean reusable gloves daily. |
| ___ | 7. Remove gloves properly. |
| ___ | 8. Wear glove liners. |
| ___ | 9. No jewelry at work. |
| ___ | 10. Long sleeves buttoned or taped inside gloves. |
| ___ | 11. Rubber boots with pants taped inside for concrete work. |
| ___ | 12. Never let cement product remain on skin or clothes. |
| ___ | 13. Avoid barrier creams. |
| ___ | 14. Avoid skin products at work. |
| ___ | 15. Change out of work clothes before leaving jobsite. |
| ___ | 16. See a doctor for any persistent skin problem. |
SURFACE SKIN pH TESTING
| Palm | pH ___ | Palm | pH ___ | Palm | pH ___ |
| Between Fingers | pH ___ | Between Fingers | pH ___ | Between Fingers | pH ___ |
| Back of Hand | pH ___ | Back of Hand | pH___ | Back of Hand | pH ___ |
| Date | ______ | Date | ____ | Date | _____ |
This questionnaire is designed specifically for Portland cement products workers. Please fill it out by placing a check mark in the box that represents the best answer. Do not worry if you cannot answer every question exactly. Remember, if possible, collect the Material Safety Data Sheets (MSDS) for the materials you work with before visiting your doctor for any skin problem.
Skin Problem History
| Yes | No | Not Sure | |
|
|
|
|
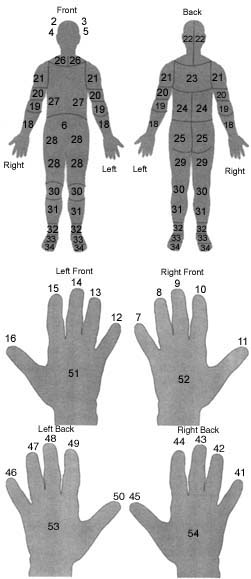
Do you currently have a skin problem? If yes, list the affected areas from the drawings:________ |
|
|
|
|
Have you had other skin problems in the past year? If yes, list the affected areas from the drawings:___________ |
| Yes | No | Not Sure | |
|
|
|
|
When the condition first appeared, did it have any of the following features? |
|
|
|
|
Rash |
|
|
|
|
Redness |
|
|
|
|
Blisters |
|
|
|
|
Fissures/cracks |
|
|
|
|
Scaling |
|
|
|
|
Oozing |
|
|
|
|
Bumps |
|
|
|
|
Other:______ |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Have you had
this kind of skin problem in past year while doing similar work?
If yes, how many times? |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Is the current problem more severe than most other problems? |
|
|
|
|
Is the current problem more widespread than most other problems? |
|
|
|
|
Has the current problem lasted longer than most other problems? |
|
|
|
|
Do you notice
any other symptoms while working with materials? Burning eyes, sneezing,
wheezing, other? (Please describe.) |
| Yes | No | Not Sure | |
|
|
|
|
Have you had a history of skin problems? |
|
|
|
|
Was it diagnosed by a doctor |
|
|
|
|
Was the causative agent or agents identified? Do you notice any other
symptoms while working with materials? (Please describe) ____________________________________ |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Was the contact dermatitis treated with over-the-counter medications? (Please Describe.) _____________________________ |
|
|
|
|
Was the contact dermatitis treated with prescription medications? (Please describe.) _____________________________ |
|
|
|
|
Did the contact dermatitis improve with any of these treatments? (Please describe.) _____________________________ |
|
|
|
|
Are you using medications for this skin problem now? (Please describe.) _____________________________ |
Work/Job History
|
What kind of work were you doing at the time or just before you developed the skin problem? |
___________________________ |
| How long have you been working at this specific job? | ___________________________ |
| How long have you been doing similar jobs? | ___________________________ |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Did these jobs involve some similar materials that contacted you skin? |
|
|
|
|
Did working with these materials ever give you a skin problem in the past? |
|
|
|
|
Are there others at work with skin problems similar to yours? |
|
|
|
|
Do any of them work with the same materials as you? |
|
|
|
|
Have there been changes in work procedures, or materials which have happened at about the same time the skin problem developed? |
|
|
|
|
Have you noticed a relationship between your work and the work occurrence of this skin problem? Which type of work? ________ |
|
|
|
|
Have you noticed a relationship between a specific work activity and this skin problem? Which activities? ___________ |
|
|
|
|
Have you noticed a relationship between working with a specific material and this skin problem? Which materials? |
|
|
|
|
Have
you detected improvements in the skin problem during changes in work
procedures, assignments, or locations? Which changes? _________________________________________ |
|
|
|
|
Have you detected worsening in the skin problem during changes in work procedures, assignments, or locations? Which changes? |
Have you detected an increase in the severity or frequency of the skin
problem with any of the following exposures?
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Exposure to materials at home or during recreational activities? |
|
|
|
|
Sweating, vigorous activity? |
|
|
|
|
Exposure to sun? |
|
|
|
|
Seasonal changes, time of day? |
|
|
|
|
Comments/other ____________________________ |
Do any of the following materials seem to cause your skin problems?
|
Yes |
No |
Not
Sure |
(Please identify products, manufactures, if possible.) |
|
|
|
|
Dry Cement ______________________________ |
|
|
|
|
Wet Cement______________________________ |
|
|
|
|
Plastic additives __________________________ |
|
|
|
|
Curing agents______________________________ |
|
|
|
|
Other additives ____________________________ |
|
|
|
|
Adhesives______________________________ |
|
|
|
|
Epoxies ______________________________ |
|
|
|
|
Finishes ______________________________ |
|
|
|
|
Others ______________________________ |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Have you noticed improvement in the skin problem during days off or vacation? If yes, how many days away from work are needed before you notice some improvement in the skin problem? |
Skin Protection
Do you keep your
skin clean and dry by wearing any of the following protective gear?
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Rubber or chemical resistant coat/apron/coveralls |
|
|
|
|
Sleeve covers? |
|
|
|
|
Rubber gloves? |
|
|
|
|
Cloth gloves? |
|
|
|
|
Leather gloves? |
|
|
|
|
Cotton gloves with butyl-dipped digints and palms? |
|
|
|
|
Other gloves? Please describe: ________________ |
|
|
|
|
Cloth coveralls? |
|
|
|
|
Eye protection/goggles? |
|
|
|
|
Face protection/mask? |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Do you use a barrier cream? |
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Do you change your skin protective gear regularly? How often, usually? |
|
|
|
|
Is this enough to keep your skin clean and dry of work materials? |
|
|
|
|
Are you able to wash your skin and change skin protective gear if material gets inside while at work? |
|
|
|
|
After material gets on your skin, are you able to wash and change protective gear within a half hour? |
Skin Cleaning
| Yes | No | Not Sure | |
|
|
|
|
Is your skin problem in an area of skin that is exposed at work? |
| How often do you usually clean off this skin while at work? | |
|
|
1-3 times daily |
|
|
4-6 times daily |
|
|
More than 6 times daily |
|
|
Not sure |
| Do you usually use any of the following for skin cleaning at work? | |||
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Tool rinse bucket water |
|
|
|
|
Drinkable running water |
|
|
|
|
Drinkable water from a tank |
|
|
|
|
Non-drinkable water from a tank or hose |
|
|
|
|
Other (please describe): ___________________ |
| Do you use any of the following for skin cleaning? | |||
|
Yes |
No |
Not
Sure |
|
|
|
|
|
Bar soap |
|
|
|
|
Liquid soap |
|
|
|
|
Detergent (dish washing or laundry) |
|
|
|
|
Waterless cleaner |
|
|
|
|
Abrasive cleaner |
|
|
|
|
Solvents/kerosine/gasoline |
|
|
|
|
Other (please describe): ___________________ |
| Do you regularly apply any of the following to your skin at home? | |||
|
|
|
|
|
|
|
|
|
Nonprescription creams/lotions |
|
|
|
|
Prescription creams |
|
|
|
|
Lanolin |
|
|
|
|
Petroleum jelly |
|
|
|
|
Neutralizing or buffering solution |
|
|
|
|
Other (Please describe): _____________ |
Other
What other kinds of work do you do? ______________________
What hobbies do you do? _______________________________
1. el Sayed, F
and J Bazex. Airborne contact dermatitis from chromatein cement with recall
dermatitis on patch testing. Contact Dermatitis Vol 30, No. 1: 58, January
1994.
A woman became sensitized to chromate from cement from her partner's work
clothing. She developed eczema in skin folds at the elbow and neck and
fissuring of fingertips. Lesions may be induced by the alkalinity and
abrasive effect of wet cement. In the present case, skin folds are sweating
areas and deposition of cement dust there may have produced an initial
irritant reaction that facilitated the penetration of chromate, thus resulting
in sensitization.
2. White, MC,
MB Larson and RD Wolford. The role of personal beliefs and social influences
as determinantis of respirator use among construction painters. Scand
J Work Environ Health 14, 239-245, 1988.
The purpose of this study was to identify and rank potential determinants
of respirator use among construction painters. As part of a health survey
of union painters, 169 male spray painters were questioned about their
own belief s concerning the consequences of wearing cartridge respirators,
as well as about the perceived attitudes of others in the work place toward
respirators. ... The most important beliefs concerned discomfort or inconvenience.
Other determinants associated with respirator use were respirator availability,
cigarette smoking, and social influences. The health belief most strongly
associated with intended respirator use was that the painter would be
able to produce healthy children if a respirator were used.
3. Avnstorp, C.
Risk factors for cement eczema. Contact Dermatitis 25: 81-88, 1991.
Risk factors for cement eczema were studied among workers employed in
the Danish construction industry. Two cohorts exposed to cement containing
different concentrations of water-soluble chromate were examined. A statistically
significant decrease in the number of workers with allergic cement eczema
was found in the cohort exposed to cement with the lower water- soluble
chromate concentration. Allergic cement eczema was found to have a greater
extent of involvement than irritant cement eczema. A 3rd cohort was followed
to evaluate individual risk factors. The degree of exposure to wet cement
seems to have a certain, though not statistically significant , effect
on the risk of developing irritant cement eczema. Individual preventive
measures, such as the use of gloves and creams, did not seem to reduce
the development of irritant cement eczema.
4. van der Valk, PGM and HI Maibach. The Irritant Contact Dermatitis Syndrome, CRC Press, Boca Ratson, 1996.
5. Klemm, WA.
Hexavalent chromium in portland cement. Cement, Concrete, and Aggregates,
CCAGPD Vol 16, No. 1: 43-47, June 1994.
...[T]he amount of hexavalent chromium found in portland cement is coming
under increasing scrutiny. Hexavalent chromium has been classified as
a carcinogen, and its release into the air or groundwater is regulated
and controlled under many federal and state regulations... As a consequence,
Scandinavian countries have limited the amount of hexavalent chromium
in Portland cement. This is generally accomplished by intergrinding clinker
and gypsum with the chemical reducing agent , ferrous sulfate, which maintains
hexavalent chromium below 2 ppm. Developments in t his area are reviewed.
Studies at a California plant showed that more than half of the hexavalent
chromium in the cement was contributed by the grinding media in the finishmill.
Attempts to reduce the chromium to its benign trivalent form with ferrous
sulfate failed in full - scaletrial grinds, due to oxidation of the ferrous
iron. This indicates that further research is needed to f i nd better
methods for introducing ferrous sulfate into the cement to develop more
stable reducing agents.
6. Larson, M,
and R Wolford, Survey of apprentice cement masons, FOF Communications.
Report to NIOSH/ CPWR Consortium 1997.
442 apprentices were surveyed using a questionnaire condensed from a version
used by NIOSH. Response rate was 100%. Mean years in industry : 3.3; mean
age: 27; most frequent age: 20.
7. International Labour Organization, Encyclopedia of Occupational Safety and Health. Geneva, 1987.
8. US DOL Bureau of Labor Statistics, reported in the Construction Chart Book, CPWR, 1998.
9. Halbert, AR
et al. Prognosis of occupational chromate dermatitis. Contact Dermatitis
27: 214-219, 1992.
To elucidate further the natural history and prognosis of occupational
chromate dermatitis, 120 affected patients, diagnosed between 1980 and
1989, were reviewed...65% of patients were construction workers with cement-induced
chromate dermatitis... The median age at onset of symptoms was 34 year,
with 48% having been exposed to chromate for 5 years or less. Only 37%
presented to the dermatologist within 12 months of developing symptoms.
76% of patients had ongoing dermatitis at the time of the review. Although
48% of the study population had completely changed their occupation to
avoid chromate exposure, symptoms persisted in 69%. A delayed diagnosis
of chromate sensitivity was noted to be a predictor of chronicity. In
view of the potential chronicity of chromate dermatitis and its associated
social and occupational impairment, we recommend the addition of ferrous
sulphate while mixing bagged cement at the work site. This simple technique
targets the workers at greatest risk of becoming sensitized.
10. Nethercott , JR and DL Holness. Disease outcome in workers with occupational skin disease. J Amer Acad Dermat ol 30:569-574, 1994.
11. Rosen RH and S Freeman. Prognosis of occupational contact dermatitis in New South Wales, Australia. Contact Dermat it is 29:88-93, 1993.
12.Wall LM and KA Gebauer. A follow-up study of occupational skin disease in Western Australia. Contact Dermatitis 24:241-243, 1991.
13. 13.Elias,
PM et al. Epidermal pathogenesis of inflammatory dermatoses. American
Journal of Contact Dermatitis Vol 10, No. 3: 119-126, September 1999.
It is generally assumed that dermatitis, whether of allergic or irritant
in origin, is primarily an immunological/inflammatory disorder. ...[R]ecent
information supports an epidermal contribution to these disorders, as
well as several other dermatoses. We first review new concepts of the
epidermal barrier , with recent evidence that the stratum corneum is a
biosensor that regulates the epidermal lipid and DNA-metabolic responses
to a variety of exogenous insults. Various signaling mechanisms, including
changes in levels of epidermal cytokines and growth factors, are potential
candidates to mediate these metabolic responses. ...[T]hese signaling
molecules may be generated not in response to permeability barrier requirements,
but as an avoidable consequence of the epidermal injury that accompanies
all types of acute barrier abrogation. Although the role of cytokines/growth
factors as regulators of metabolic events leading to barrier recovery
is still unknown, their role initiating a cytokine cascade leading to
cut aneous pathology seems more certain. We conclude that signaling molecules,
released following injury to the stratum corneum, initiate a cytokine
cascade that induces inflammation, which is responsible for the clinical
features of specific dermatoses. Thus, ‘outside-to-i nside’
signaling may contribute to the pathogenesis of a variety of dermatoses
characterized by abnormal barrier function.
14.Elias, PM et al., Relationship of the epidermal permeability barrier to irritant contact dermatitis, Immunology and Allergy Clinics of North America, Vol. 17 (Contact Dermatitis: Irritant and Allergic) Philadelphia, PA, W.B. Saunders, 1997, pp. 417-430.
15.Mauro, T et
al. Barrier recovery is impeded at neutral pH, independent of ionic effects:
implications for extracellular lipid processing, Arch Dermat ol Res, 290:215-222,
1998.
Epidermal permeability barrier homeostasis requires the post secretory
processing of polar lipid precursors into nonpolar lipid products within
the stratum corneum (SC) interstices by a family of lipid hydrolases.
A specific requirement for B-glucocerebrosidase, which exhibits a distinct
acidic pH optimum, is particularly well documented. Therefore, we sought
to determine whether the recovery of the barrier after acute insults requires
acidification of the SC. We examined permeability barrier recovery by
assessing changes in transepidermal water loss (TEWL), SC membrane ultrastructure
... at an acidic vs neutral pH. Barrier recovery proceeded normally when
acetone-treated skin was exposed to solutions buffered to an acidic pH.
In contrast, the initiation of barrier recovery was slowed when treated
skin was exposed to neutral or alkaline pH, regardless of buffer composition.
...These results suggest first that an acidic exracellular pH is necessary
for initiation of barrier recovery, and second that the delay in barrier
recovery is a consequence of inhibition of post secretory lipid processing.
16.Goh, CL et
al. Occupational dermatitis in a prefabrication construcion factory. Contact
Dermatitis Vol 15, No. 4: 235-240, October 1986.
In a field study of occupational dermatoses in a prefabrication construction
factory , 272 workers were interviewed, examined and patch tested to chromate,
cobalt , nickel , rubber mixes, epoxy resin, melamine formal dehyde and
conplasts. The prevalence of occupational dermatitis was 14% (38/272)
; 57% (22/38) were irritant dermatitis from cement ; 39.5% (15/38) were
allergic contact dermatitis from cement (2 with concomitant rubber glove
allergy) ; and 2.5% (1/38) were allergic to rubber chemicals in gloves.
The overall prevalence of chromate sensitivity was 8.5% (23/ 272) , with
the highest rate from the concreting bays of the factory. The rate was
unrelated to the duration of workers engagement in construction work.
34. (/23) had asymptomatic chromate allergy. The prevalence of cobalt
reactions was 1.4 (4/23) and all were associated with chromate allergy.
17. Denda, M et
al., Exposure to a dry environment enhances epidermal permeability barrier
function. J Invest Dermatol, 111:858-863, 1998.
Previous studies have suggested that transepidermal water movement
may play an important role in epidermal homeostatis and barrier repair.
Here we analyzed cutaneous barrier function, epidermal morphology, and
lipid content of the stratum corneum in hairless mice maintained in a
high relative humidity (R H 0) versus low humidity (RH 10) environment
for 2 wk. Basal transepidermal water loss was reduced by 31 in animals
maintained in a dry versus humid environment... furthermore, the dry weight
of the stratum corneum and the thickness of the epidermis also increased
in a dry environment...
18. Avnstorp,
C. Prevalence of cement eczema in Denmark before and since addition of
ferrous sulfate to Danish cement. Act a Derm Venereol, Vol 69, No. 2:
151-155, 1989.
This is a study of the prevalence of chromate allergy and hand eczema
among workers engaged in the manufacture of prefabricated concrete building
components in Denmark in 1981 and again in 1987. In September 1981 the
chromate content of cement manufactured and sold in Denmark was reduced
to not more than 2 ppm (parts per million) of water-soluble chromate.
This was accomplished by adding ferrous sulfate, thus increasing the cost
of the cement by about 1%. There was a statistically significant decrease
in the prevalence of chromate allergy and hand eczema following the addition
offerrous sulfate, but there was no change in the frequency of skin irritation.
The economic benefit of adding ferrous sulfate was demonstrated by a decrease
in the need for dermatological services and topical steroid treatment.
Cement eczema as a result of chromate allergyis a common occupational
dermatitis among workers in the building and construction industries and
a reduction in the chromate content of cement would appear to be a reasonable
preventive measure in areas where there is a large concentration of construction
industries.
19.Wolford, R
and M Larson, pH testing of cement-exposed skin, American Industrial Hygiene
Association Annual Conference, May 2000.
This field study examined the effectiveness of gloves, water rinses, and
pH- neutralizing agents in controlling alkaline cement residue on palmar
skin of 27 concrete finishers at five locations in four states. Full range
pH indicator papers and meters were used to measure palmar skin pH. After
two hours of work, mean palmar skin pH of workers not wearing gloves was
9.9. This did not differ significantly from the mean pH of workers wearing
leather gloves, cloth gloves, or rubber gloves. Workers subsequently attempted
to decontaminate skin through the usual practice of rinsing hands in tool
rinse buckets. Prerinse, mean palmar skin pH was 10.4. After rinsing,
mean palmar pH was 9.3. Addition of a phosphate buffering agent to the
rinse water significantly reduced palmar pH from a prewash mean of 10.4
t o 5.9.
20. Portland Cement Association. Report of sample material safety data sheet for portland cement . Skokie, IL, 1997.
21.Feldberg, L
et al. Cement burns and their treatment. Burns Vol 18, No. 1: 51-53, 1992.
Trying to discover why people with full skin thickness burns did not immediately
report these burns, authors reviewed 20 cases at a hospital in Buckinghamshire,
UK. 15 had occupations in which they might be expected to come into contact
with wet cement. 50% of burns were on ankles. 80% had full skin thickness
burns and 75% under went wound excision and grafting. Time from injury
to presentation at the hospital varied from a few hours to 10 days. Treatment
recommendations for injured person as well as for doctors.
22.Wolford, R
and M Larson, Efficacy of buffering solution as a protectant for workers
using alkalies. Abstract . Am J Contact Dermatitis, Vol. 11, No. 2, June
2000.
This is an assessment of the efficacy of a pH 5.5 buffering rinse to improve
the condition of skin occupationally exposed to alkalies, compared with
water washing, moisturizers, and gloves. Pre/posttreatment surveys of
30 concrete truck drivers were completed 30 days apart . Workers reported
daily on use of the four treatments and were grouped by treatment compliance
(high/low). Relative risk for skin improvement was estimated between compliance
groups. Workers using buffering rinse were 7.8 times more likely than
workers not using it to report improvement. No differences were seen between
workers using and not using water washes, moisturizers, or gloves. No
difference in reported frequency of symptoms was seen between compliance
groups for any treatment.
23.Bruze, M et al. Patch testing with cement containing iron sulfate.
Dermatol Clin Vol 8, No. 1: 173-6, January 1990.
Addition of iron sulfate to cement means transformation of water - soluble
hexavalent chromium into nonwater-soluble trivalent chromium. This has
been the basis for preventive measures concerning sensitization to hexavalent
chromium (chromate) in cement . For some years, iron sulfate has been
added to cement manufactured in the Scandinavian countries. In the present
in vivo study, cements with and without iron sulfate were compared concerning
their capacity to elicit allergic patch-test reactions in eight chromate-hypersensitive
individuals. No patch-test reactions were obtained from a water extract
of cement with iron sulfate when appropriately buffered.
24. Fregert, S et al. Reduction of chromate in cement by iron sulfate.
Contact Dermatitis VOl 5: 39-42, 1979
Cement dermatitis is connected with chromate sensitivity...Iron sulfate
added to cement reduces the chromate completely, and the 3-valent chromium
is precipitated. An amount of 0.35% (w/w) iron sulfate, FeSo.7H0, is enough
to reduce 20 micrograms Cr
6+
/g cement. There is no technical side effect to the concrete. Iron sulfate
is preferably added to cement when there is an intimate contact with skin,
e.g., at floor laying, repairs and handmade casting.
25. Goh, CL and SL Gan. Change in cement manufacturing process, a cause
for decline in chromate allergy? Contact Dermatitis Vol 34, No 1: 51-54,
January 1996
Hexavalent chromate in cement is the commonest cause of allergic dermatitis,
especially among construction workers. Over the past decades, there has
been a general decline in the prevalence of chromate allergy among construction
workers. We suspect that a change in the constituents of cement, resulting
in the lowering of hexavalent chromate, contributed to the decline. Slag
(free from hexavalent chromate) from the iron-quenched, blast furnace
process has been used as a substitute for clinker (which contains high
hexavalent chromate) in manufacturing cement. As a result, the slag has
diluted the hexavalent chromate content of cement. Our analytical study
showed that slag is free from hexavalent chromate and that he hexavalent
chromate of clinker ranged from 6-17 micrograms/s. Substituting slag for
clinker resulted in dilution of hexavalent chromate in the cement. The
hexavalent chromate content of cement declines proportionately with increasing
proportion of slag.
26.Goh, CL and SF Kwok. Prevention of cement dermatitis in construction
workers with iron sulphate. Asia-pacific Journal of Public Health. Vol
1, No. 1: 91-93, 1987.
Allergic dermatitis due to chromate in cement is the most common occupational
dermatitis among construction workers in Singapore. Hexavalent chromate
in cement can be removed by iron sulphate. This study determined the minimum
concentration of iron sulphate required to remove the hexavalent chromate
from nine brands of Asian cement. The hexavalent chromate concentrations
in cements were determined by colorimetric spectrophotometry. The minimum
amount of iron sulphate required to remove completely hexavalent chromium
in all the cements was 0.35% w/w. Iron sulphate should be used in the
construction industry to prevent cement dermatitis in construction workers.
27. Avnstorp, C. Follow-up of workers from the prefabricated concrete
industry after the addition of ferrous sulphate to Danish cement. Contact
Dermatitis Vol 20, No. 5: 365-371, May 1989.
Ferrous sulfate has been added to cement manufactured in Denmark, reducing
the water soluble chromate content to not more than 2 ppm, since September
1981. A comparison is made between the medical and employment status of
a cohort of workers engaged, or who had been engaged, in the manufacture
of prefabricate concrete building components in 1981 and in 1987. Workers
who had allergic cement eczema in 1981 appeared to show no improvement
6 years after the reduction of chromate in the cement. Improvement was
seen, however, in the eczema of those workers with irritant cement eczema.
The 1987 study showed that a larger number of chromate-sensitized workers
required medical services and topical steroid treatment than did those
who were not sensitized to chromate. This difference was statistically
significant. The worse medical prognosis of the chromate-sensitized workers
could in part be due to the fact that some of these had secondary contact
sensitivity to cobalt and rubber chemicals. The chromate-sensitized workers
also took earlier retirement. Younger workers with allergic and irritant
cement eczema continued to work and their employment status was not influenced
by chromate sensitization.
28. Kolbe, L. Enhancement of the stratum corneum barrier: the effect
of moisturizer treatment, American Contact Dermatitis Society Annual Meeting,
March 1999.
We studied the effect of moisturizers on the barrier function of the
skin and the susceptibility to irritants after treatment...Moisturizers
are thought to act by increasing the amount of water within the stratum
corneum and have no long-lasting effects. However, our studies provide
evidence that moisturizers help to sustain a healthy horny layer, assist
to repair an impaired stratum corneum barrier, and prevent the development
of irritant dermatitis. (Author's Note: The moisturizer found effective
in this study was Nivea Cream, widely available in drug stores)
29. Goh, CL. Common industrial processes and occupational irritants and
allergens: an update. Ann Acad Med Singapore Vol 23, No. 5: 690-698, September
1994.
This paper reviews the recent development of the industrial processes
in the construction, electronics and metal industries which are the predominant
industries in developing countries.. The information is essential for
occupational dermatologists and physicians managing patients with occupation
skin diseases. In the construction industry, the prefabrication construction
methods are now widely used. The commonest irritant is cement and the
allergens are chromate, rubber chemicals and epoxy resins...Preventive
measures including health education are most effective against occupation
dermatitis.
30. Cooley, J and JR Nethercott. Prognosis of occupational skin disease.
Occupational Medicine: State of the Art Reviews Vol 9, No. 1: 19-25, January-March
1994.
The prognosis in occupational skin disease (OSD), which is largely irritant
(ICD) and allergic contact dermatitis (ACD), is guarded. Many investigations
over the last five decades have documented that a large portion of workers
developing such disease do not improve with present methods of secondary
preventive intervention and treatment. Although cases of ACD may do better
when a specific cause can be found and avoided, ACD due to the metals
nickel and chromium has a poor prognosis. Job changes are of equivocal
value. Early diagnosis and intervention are associated with a better prognosis
for cure. Medical management alone has not modified the outcome significantly
over the last decade. Greater attention to primary prevention through
regulation of exposure to irritants and sensitizers, combined with more
effective measures for control of control of industrial hygiene, offers
the possibility of more effective management.
31. Buckley, DB. Skin burns due to wet cement. Contact Dermatitis 8:
407-409, 1982
Four cases of cement burns from prolonged contact with wet cement, one
requiring skin grafting. Includes recommendations for treatment (flushing
area with water or diluted vinegar until soapy feeling is gone), and prevention
(notices on cement bags and handed to purchasers, kneel on board, watertight
boots tied at top to be in close contact with the skin.
32. Fisher, AA. Cement injuries: Part II. Cement burns resulting in
necrotic ulcers due to kneeling on wet cement [news]. Cutis Vol 61, No.
3: 121, March 1998.
33. Pike, J et al. Chemistry of cement burns: pathogenesis and treatment.
JBCR Vol 9, No. 3: 258-260, May/June 1988.
Two brief cases are presented describing burns resulting from exposure
to cement and its components.
34. Goh, CL. Sickness absence due to occupational dermatoses in a prefabrication
construction factory. Contact Dermatitis Vol 15: 28-31, 1986.
In a study of sickness absence due to occupational dermatoses among 360
construction workers in a prefabrication construction factory in 1984,
we found 3 workers with allergic contact dermatitis from chromate in cement
who required medical leave. There were 5 sickness absence spells due to
occupational dermatoses and the number of days lost due to occupational
dermatoses was 53 days fro the year. This averaged out at 0.01 spells
per worker per year, 0.15 per worker per year and 15 days per spell. It
appeared that the number of workers requiring sickness absence from occupational
dermatoses was low, but that those with the condition required about 2
weeks of sickness absence. Allergic contact dermatitis from chromate in
cement appeared to be the only occupational dermatosis causing sickness
absence in the factory.
35. Lushniak, BD. The public health impact of irritant contact dermatitis.
Immunology and Allergy Clinics of North America Vol. 17, No. 3: 345-358,
August 1997.
36. Lushniak, BD. Epidemiology of occupational contact dermatitis. Dermatologic
Clinics Vol 13, No. 3:671-680, July 1995.
37. Meherin, JM, and TP Schomaker. The cement burn: Its etiology, pathology
and treatment. Jour. A.M.A. No. 14: 1322-1326, April 8, 1939, Microscopic
pictures of burn progression damage.
38. Roto, P, et al. Addiction of ferrous sulfate to cement and risk of
chromium dermatitis among construction workers. Contact Dermatitis, 34(1):43-50,
January 1996
39. Wigger-Alberti, W and P Elsner. Do barrier creams and gloves prevent
or provoke contact dermatitis. Am J Contact Dermatitis, Vol. 9, No. 2,
June 1998.
40. De Raeve, H et al. Dermal and respiratory sensitization to chromate
in a cement floorer. Am J Ind Med Vol 34, No. 2: 169-176, August 1998.
A 48-year old floorer, occupationally exposed to cement and with a documented
chromate contact dermatitis, reported dyspnea and wheezing after work.
These conditions were demonstrated by self-measured sequential peak expiratory
flows..This report illustrates that a subject, with allergic contact dermatitis
to chromates, may develop a respiratory allergic reaction to an airborne
source of this metal.