
Worker Fatigue: Managing concerns in rapid renewal highway construction projects
Summary Statement
Study of the impact of rapid renewal projects and nighttime work on workers and injury rates and steps to identify and manage fatigue and reduce injuries.
December 2010
 Matthew R. Hallowell, Ph.D., is an assistant professor in the Department of Civil, Environmental and Architectural Engineering at the University of Colorado, Boulder. He holds a B.S. and an M.S. from Bucknell University and a Ph.D. in Civil Engineering from Oregon State University. A professional member of ASSE’s Colorado Chapter, he is a member of ASSE’s Technical Publications Advisory Committee, the CII Safety Community of Practice, and the ASCE Site Safety and Prevention Through Design committees.
Matthew R. Hallowell, Ph.D., is an assistant professor in the Department of Civil, Environmental and Architectural Engineering at the University of Colorado, Boulder. He holds a B.S. and an M.S. from Bucknell University and a Ph.D. in Civil Engineering from Oregon State University. A professional member of ASSE’s Colorado Chapter, he is a member of ASSE’s Technical Publications Advisory Committee, the CII Safety Community of Practice, and the ASCE Site Safety and Prevention Through Design committees.
HIGHWAY CONSTRUCTION WORK can be demanding and exhausting. It requires intense focus and physical exertion, the use of heavy mobile equipment and repetitive work tasks, and it is performed adjacent to traffic (NIOSH, 2001). These factors all contribute to the relatively high injury rate in the construction sector (BLS, 2007).
Traditionally, roadway construction has been performed during normal, daytime work hours. However, as America’s highway infrastructure continues to degrade and congestion becomes an increasing concern, roadways must be renewed quickly
As a result, rapid renewal strategies such as nighttime work, continuous work, extended shifts and modularization are employed to compress schedules and minimize traffic disruption (Transportation Research Board, 2009). While these strategies enhance overall schedule performance, the associated conditions contribute to worker fatigue, which compounds the safety risk factors inherent to highway construction.
Rapid renewal projects are especially susceptible to two types of fatigue: cognitive fatigue and localized muscular fatigue. Cognitive fatigue is the lassitude of thought and decision processes, while localized muscular fatigue is the reduction in peak tension of a specific muscle group due to prolonged or excessive use.
Researchers have found that conditions in work environments similar to rapid renewal projects contribute to both types of fatigue because construction laborers perform repetitive tasks for extended work shifts and must continuously communicate with the other crew members while performing complex, dynamic and fast-paced work (Sauer, Wastell, Hockey, et al., 2002; Matthews & Desmond, 1998).
However, few available references promote effective fatigue management on construction projects and no literature focuses on rapid renewal scenarios. This article summarizes the relatively large but disparate body of literature related to mental and localized muscular fatigue and offers a conceptual model for fatigue management on highway construction projects.
| Abstract: Construction strategies that minimize congestion and disruption to local communities are becoming more common. These rapid renewal strategies involve extended work shifts, nighttime work and work zones adjacent to active roadways. Since rapid renewal will likely add to occupational fatigue on highway construction sites, managers must understand occupational fatigue to successfully deliver projects with minimal injuries. This article reviews characteristics that contribute to cognitive and localized muscular fatigue, methods to measure and control fatigue and its effects on safe work behavior and quality of life. A model of fatigue management is offered as well. |
Rapid Renewal
Simply stated, rapid renewal means completing highway projects quickly, with minimal disruption to the community and producing facilities that are long lasting. Rapid renewal applies innovative techniques or technologies to reduce the time traditionally allocated to on-roadway activities.
Benefits of this approach include minimizing disruptions to the traveling public, business owners and communities. These benefits are realized in the form of fewer delays, shorter periods with reduced capacity roadways and less construction noise. On the downside, such scenarios may affect worker fatigue and may indirectly compromise worker safety and health, productivity, quality and teamwork. Persons affected may include designers, construction managers, inspectors, laborers and others.
Specific Rapid Renewal Tactics
Some confusion exists regarding the specific tactics that characterize rapid renewal projects. Recently, Transportation Research Board (2009) identified several tactics developed to reduce the time needed to complete on-roadway construction:
- Perform faster in situ construction by performing projects on a compressed schedule. To achieve this, contractors extend overtime shifts, mobilize additional workers, and employ innovative technologies and strategic design. This tactic also typically involves the use of design-build project delivery, flexible performance specifications and nondestructive testing.
- Minimize field fabrication and maximize prefabrication that can occur off site. This tactic may entail prefabricating units of roadway or bridges, modular construction and innovative installation strategies. Modular and prefabricated elements allow for accelerated schedules, improved quality control and longevity; such techniques also enhance the project’s overall level of performance.
- Perform faster construction inspection and monitoring by ensuring that renewal projects are inspected and accepted quickly so that they may be reopened to the public.
- Facilitate innovative and equitable contracting environment by making decisions and accepting them rapidly. To effectively employ this tactic, risk must be shared among project partners (e.g., DOT agencies, designers, private contractors, partners). Additionally, performance-based specifications must be used to give the contractor control over construction- related risks.
- Improve customer relations by recognizing the role that utilities and railroads play in project development and execution. To prevent conflicts, institutional and procedural changes must be made and a proactive strategy for dealing with conflicts must be established early on.
The most common rapid renewal tactics involve the use of management strategies that compress construction schedules. These strategies focus on altering construction means and methods, work shift duration and the intensity of critical phases. As noted, use of these strategies can increase worker fatigue, thereby affecting work zone safety and the workforce’s quality of life.
Let’s review causal factors of fatigue in general; individual risk factors; immediate effects on safety, health and human error; effects on work performance; long-term effects; methods of measuring fatigue; and known countermeasures.
Occupational Fatigue
Fatigue, defined as lassitude or exhaustion of mental and physical strength resulting from bodily labor or mental exertion, is a concern of workers in many occupations throughout the world. While occupational safety and health has improved in recent decades, fatigue remains a common problem in developed countries (Lewis &Wessely, 1992).
Fatigue is a serious threat to quality of life and severely compromises work performance when it becomes chronic or excessive (Piper, 1989; Okogbaa, Shell & Filipusic, 1994). Unfortunately, its complex and dynamic nature makes fatigue difficult to define, observe and measure. As a result, it has traditionally been excluded by funding agencies and scientific studies, especially in construction.
While few studies have examined fatigue in the construction industry, a wide body of literature describes the general causes and effects of occupational fatigue. It is assumed that research from industries such as manufacturing and transportation apply to the infrastructure construction environment because of the prevalence of repetitive work tasks, use of heavy equipment and complex work processes. That said, some characteristics of construction, such as exposure to the elements and dynamic work environments, may not be adequately modeled in previous research in other industries.
To classify the types of fatigue that occur in occupational environments, Bills (1934) established definitions and distinctions for three types of fatigue: physiological (reduction of physical capacity), objective (reduction in work) and subjective (feelings of weariness). Secondary aspects of fatigue include sleepiness (Gillberg, Kecklund & Akerstedt, 1994), discomfort, and weakened activation and weakened motivation (Kashiwagi, 1969).
These essential studies provide the framework for fatigue research and for the development of objective measures. While little fundamental or transformative research has been performed in recent decades,many studies have refined this fundamental body of literature and have explored fatigue in specific industries and emerging work scenarios (Leung, Chan, Ng, et al., 2006; Jansen, van Amelsvoort, Kristensen, et al., 2003; Ashburg, Gamberale & Kjellberg, 1997).
Causal Factors
Various factors can contribute to cognitive and localized physical fatigue, including specific occupational activities, recreational activities, personal characteristics, drug use, sleep deprivation and physical condition. Managers must understand the signals of these types of fatigue as a careful analysis can identify high-risk individuals and work environments. While many factors affect fatigue, the threemajor factors related to rapid renewal highway projects are shift work, extended work shifts and work time control.
During rapid renewal projects, workers often must adapt to new work shifts, extended shifts and high intensity work. While the effects of such transitions have yet to be explored in the construction industry, a large body of literature discusses the effects of shift work on fatigue in manufacturing settings. It is expected that many of these underlying principles apply to rapid renewal highway projects despite the obvious differences between manufacturing and construction.
Findings from several fundamental studies are concisely presented as follows:
- Andlauer (1960), Bruusgaard (1969) and Akerstedt (1988) estimated that about 20% of the worker population is unable to adapt to shift work.
- Adaptation to shiftwork occursmore easily and more often in “stabilized” rather than “rotating” shifts (Colquhoun, 1971).
- Well-adapted shift workers show significantly less psychosomatic tension than poorly adapted workers (Hakkinen, 1969).
- Frequent alternation of shifts on continuous work was preferred to the commonly used 1-week spells, due to reduced experience of fatigue and monotony (Walker, 1966).
- Workers on continuous alternating shifts starting at the hours 4-12-20 obtained more sleep than after a change to 6-14-22 (Bjerner, Holm & Swensson, 1948).
- When compared with the 6-14-22 system, the 7- 15-23 system results in fewer accidents and greater productivity (Oginski, 1966;Wild & Theis, 1967).
- Fatigue is reduced when shifts occur in the order night-evening-day, instead of the more common day evening- night pattern (Saito & Kashiwagi, 1970).
Most of this foundational work was conducted in themid-20th century. Researchers have more recently investigated fatigue in complex and emerging environments such as high-speed maritime operations (Leung, et al., 2006), aviation and aerospace (Folkard & Akerstedt, 2004).
Review of this fundamental literature indicates that work shift design may significantly affect the potential for fatigue that the construction industry must recognize. Many individual factors, such as age, health and living conditions, influence a worker’s ability to adapt to shift work or changes in shift sequences, timing or duration. Likewise, extended work shifts and overtime introduce unique fatigue issues. Shift design strategies are essential to preventing both mental and localized physical fatigue.
Long work hours are common in every major U.S. industry, including construction. In fact, more than one-quarter of U.S. men and 11% of women work more than 50 hours a week (Jacobs & Gerson, 2004). In this context, extended work shifts and the term overtime refer to a prolonged investment of effort (by individual or crew) where recovery time is reduced.
The effect of extended work shifts is highlighted because long working hours can negatively affect workers’ health and well-being (Sparks, Cooper, Fried, et al., 1997; van der Hulst, 2003). Overtime work can lead to a situation of prolonged, insufficient recovery that is assumed to disturb physiological processes and, as a consequence, induce health problems (Geurts & Sonnentag, 2006).
However, the association between overtime and well-being depends on the psychosocial profile of the overtime job (Beckers, van der Linden, Smulders, et al., 2004). For example, van der Hulst (2003) shows that moderate overtime hours were only related to fatigue in cases of high job demands in combination with low autonomy.
Not all workers report ill effects from working extended periods. In fact, multiple individual characteristics, such as strong physical condition, allow some to better adjust to extended work periods. Interestingly, two psychosocial work characteristics have been found to influence overtime’s effect on fatigue and worker health: 1) control over overtime work; and 2) rewards for overtime work (Harma, 2006). Work time control has been defined as “an employee’s possibilities of control over the duration, position and distribution of work time” and reward systems include compensation for working extended hours (Harma).
Involuntary overtime work is associated with relatively high fatigue and low satisfaction, especially for involuntary overtime workers without rewards (Beckers, et al., 2004). Fenwick and Tausig (2001) found that lack of schedule control is associated with work-home interference, burnout symptoms, distress, dissatisfaction, poor general health and minor physical problems.
A series of longitudinal studies found that low work time control increases the risk of health problems, whereas high control over working time reduces the adverse effect of work stress on sickness absence and can help employees establish an appropriate work-life balance (Ala-Mursula, Vahtera, Kivimaki, et al., 2002; Ala-Mursula, Vahtera, Pentti, et al., 2004;Ala-Mursula, Vahtera, Linna, et al., 2005; Ala-Mursula, Vahtera, Kouvonen, et al., 2006).
Tucker and Rutherford (2005) found overtime work to be related to impaired health only among respondents who worked overtime in response to pressure (i.e., low overtime control) and who lacked social support. Voluntary overtime workers in comparable positions were nonfatigued and satisfied, even without rewards.
Rewards for overtime work (e.g., receiving or not receiving compensation for extra work hours) constitute another psychosocial work characteristic that may act as a moderator in the overtime/well-being association. The importance of rewards follows from the effort-reward imbalance (ERI) model (Siegrist, 1996; 1998). This theory states that employees’ efforts at work are part of a social exchange process in which employees expect fair rewards or compensation for their invested efforts. Therefore, it may be concluded that control of overtime is important for well-being and that the negative effects of compulsory overtime may be partly offset by fair compensation for the extra work (Beckers, et al., 2004).
Individual Risk Factors
All workers have unique physical conditions, intellectual abilities and emotional stability. These characteristics are manifested in the ability to adapt to extended work periods and rotating shifts, tolerance of fatigue and effects of fatigue. Age is one of the most influential factors. Thüs-Evensen (1958) recommended that workers over age 50 with no previous shift work experience be rejected because of their susceptibility to muscular fatigue. Menzel (1962) added that workers younger than age 25 are at high risk for cognitive fatigue, especially if they have to provide their own meals.
Mott,Mann,McLoughlin, et al. (1965), concluded that adapting to shift work is more difficult for younger, better educated workers who have small children,while men who could work additional jobs (“moonlighters”) seldom complained about the adaptation of their time-oriented body functions. This implies that some workers may be resistant to cognitive fatigue.
Literature has consistently shown that nearly all workers are vulnerable to localized muscular fatigue when performing repetitive tasks for extended periods. McGirr (1966) notes several conditions that should preclude employees from alternating shift work such as a need for continuous drug therapy; epilepsy or diabetes; serious gastrointestinal diseases (e.g., ulcer and colitis); heart and circulatory diseases; and marked stress and anxiety syndromes.
Many studies have also found that circadian rhythms can affect a worker’s ability to adapt. Patkai (1971) studied habitual “morning” and “evening” workers and found many significant differences in alertness, performance and adrenal excretion. She found that habitual working habits might be an important factor in determining both efficiency of performance and work satisfaction.
Ostberg (1973) estimated that the morning types are approximately 2 hours ahead of the evening types in the circadian rhythms of oral temperature and food intake. Finally,Aanonsen (1964) found that a high proportion of workers who had transferred to nonshift work for medical reasons were the early-to-bed/early-to-rise type. Table 1 presents a summary of the leading indicators for cognitive and localized muscular fatigue. Some factors are unique to either cognitive or muscular fatigue, while other factors, such as extended work periods and heat, contribute to both.
Measuring Fatigue
Researchers often report that they omit fatigue in occupational safety and health studies because it is difficult to measure and track fatigue in dynamic work environments. In the past decade, several methods for measuring fatigue have been developed, validated and vetted by the research community. Of these methods, the Swedish Occupational Fatigue Inventory (SOFI) and the similar CIS20R appear in most peer-reviewed academic publications that attempt to measure fatigue in an occupational setting.
Table 1. Leading indications for fatigue
| Causal factors | Individual risk factors |
| Long work hours (overtime) | Unsatisfactory housing conditions |
| Job with low autonomy | > 50 years of age |
| Psychosocial profile of the work | < 25 years of age |
| Low job satisfaction | Workers who must provide their own meals |
| Low control over overtime | Need for drug therapy |
| Extended work periods | Epilepsy |
| Noise | Diabetes |
| Heat | Gastrointestinal Diseases (ulcers, colitis) |
| Repetitive work tasks | Heart/circulatory diseases |
| Tasks that lead to higher VO2Max | Stress/anxiety syndromes |
| Workers with young children | |
| Early-to-bed/early-to-rise | |
| Introverts | |
| Nonrobust individuals | |
| Ill-adapted individuals |
Other measurement methods have been developed as well, but they have little application to occupational settings. For example, the use of VO2Max testing (i.e., a measure of oxygen uptake by the human body that measures aerobic capacity) would be impractical in a rapid renewal environment as it is intrusive, limits workers’ ability to remain productive and may extend work periods even further.
| Some leading indicators for cognitive and localized muscular fatigue are unique to either cognitive or muscular fatigue, while other factors, such as extended work periods and heat, contribute to both. |
To simultaneously evaluate the intensity and quality of perceived fatigue, several scales have been developed (Kinsman & Weiser, 1976). These dimensions have been labeled as lack of energy, physical exertion, physical discomfort, lack of motivation and sleepiness. The underlying structure of the instrument corresponds to a qualitative and quantitative description of the physical (exertion and discomfort) and mental (lack of motivation and sleepiness) dimensions of perceived fatigue.
Originally, the SOFI included 25 expressions (five for each dimension) related to physiological, cognitive, motor and emotional responses (Ashburg, et al., 1997). In most studies, participants were asked to rate on a 25-point scale the extent to which the expressions described their feelings at that moment, during the last few minutes, when they were most tired and so on to quantify their relative level of fatigue.
The SOFI scale has been refined and validated for occupations such as teachers, firefighters, cashiers, bus drivers and engineers. Internal consistency of the subscales was satisfactory, with Cronbach’s alphas above .80, especially for lack of energy (.92); lack of motivation (.92); sleepiness (.89); physical discomfort (.81); and physical exertion (.87). It should be noted that these scales measure whole body fatigue which includes most subsets of fatigue such as psychological fatigue, sleepiness and loss of motivation (e.g., burnout) in addition to those types highlighted in this article. Figure 1 presents the SOFI scale.
Figure 1. SOFI Scale
| Not at all To a very high degree | |||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | |
| Lack of energy | |||||||
| Worn out | |||||||
| spent | |||||||
| Drained | |||||||
| Overworked | |||||||
| Physical exertion | |||||||
| Palpitations | |||||||
| Sweaty | |||||||
| Out of breath | |||||||
| Breathing heavily | |||||||
| Physical discomfort | |||||||
| Tense muscles | |||||||
| Numbness | |||||||
| Stiff joints | |||||||
| Aching | |||||||
| Lack of motivation | |||||||
| Lack of concern | |||||||
| Passive | |||||||
| Indifferent | |||||||
| Uninterested | |||||||
| Sleepiness | |||||||
| Falling asleep | |||||||
| Drowsy | |||||||
| Yawning | |||||||
| Sleepy | |||||||
Effects of Fatigue
Safety & Work Performance
| In the past decade, several methods for measuring fatigue have been developed, validated and vetted by the research community, including the Swedish Occupational Fatigue Inventory (SOFI). |
The effects of cognitive and muscular fatigue on individual workers can cause immediate reductions in safe work behavior, productivity, teamwork and morale. Goldenhar, Hecker,Moir, et al. (2003), found that excessive overtime both within 1 day and across many days adversely affects productivity and that worker productivity was affected by the manner in which overtime jobs were run in terms of timelines and type of supervision. Goldenhar, et al., also observed that injury frequency and severity increases during extended periods of work, sometimes dramatically due to an increase in human error caused by lassitude in cognitive processes. These observations were strictly qualitative as no attempt was made to measure productivity.
Human Error
To better understand the relationship between fatigue and safe work behavior, let’s examine the potential effects of cognitive fatigue on human error. While these may seem like disparate topics, accidents, rework, conflicts and decreases in productivity involve some element of human error. According to fundamental social psychology literature summarized by Reason (1990), these errors are caused by deficiencies in mental function that are accelerated as mental and physical fatigue increase. The sidebar below lists the immediate effects of fatigue.
Errors in judgment, decision making and physical actions result in loss of productivity, the need for rework in industrial operations and occupational injuries. To prevent human error, organizations conduct training, provide feedback to workers and perform inspections (Hinze, 2006). These activities rarely involve methods to reduce or even address cognitive fatigue despite its obvious effect on thought processes.
Error Types & Potential Controls
To target human error, the various modes by which it occurs and the contribution of fatigue to each mode must be explored. According to Reason (1990), human error occurs in a limited number of forms. These include intentional erroneous actions (mistakes and violations) and unintentional erroneous actions (slips and lapses). The fundamental difference between these is that mistakes are planning errors (e.g., intentionally choosing an unsafe pathway through a worksite) while slips and lapses are the result of failures in execution (e.g., inattentiveness, distraction).
Immediate Effects of Fatigue on Humans
|
Much social psychology literature has attempted to define error types and potential controls. Let’s briefly discuss this body of literature.
Reason (1990) defines mistakes as “deficiencies or failures in the judgmental and/or inferential process involved in the selection of an objective or in the specification of the means to achieve it, irrespective of whether or not the actions directed by this decision scheme run according to plan.” According to Rasmussen, Pejtersen and Goldstein (1994), mistakes are relatively common and exist in two categories: knowledge-based or rule-based. Rule-based mistakes involve the intentional application of a bad rule. These mistakes result from errors in standardized procedures and reflect deficiencies in management.
Reason (1990) defines slips and lapses as “errors which result from some failure in the execution and/or storage stage of an action sequence, regardless of whether or not the plan which guided them was adequate to achieve its objective.” These errors occur when workers fail to make a cognitive attentional check because 1) the process or behavior is not habitual (strong habitual intrusions); 2) a distraction prevents one from making required checks (omission); 3) failures of prospective memory prevent safe work procedures (reduced intentionality); or 4) workers inadequately estimate durations within a sequence of actions (mistimed checks). These unintentional errors are differentiated into two categories, those caused by distractions in a familiar work environment (slips) and memory failures (lapses).
Knowledge-based errors are not likely to be largely affected by fatigue unless safety training and orientation meetings are conducted at times when workers are at risk of being fatigued because knowledge-based errors occur when employees do not know or understand the correct methods of performing the work. Mental fatigue is likely to have a significant impact on slips and lapses because these errors are generally caused by errors or inefficiencies in cognitive processes during specific instances in time.
Typically, errors are detected through formal processes in the human body (i.e., self monitoring). Humans constantly check their surroundings to ensure that actions match intent. As cognitive fatigue increases,workers’ ability to rapidly perform these mental checks decreases and the speed at which decision processes are executed is reduced.
According to Reason (1990), attention can only be directed to a small part of a total space in any given time and such attention must be focused on important problem spaces to prevent accidents. Such focus decreases substantially as workers become mentally fatigued. Table 2 provides simple definitions of the three human error modes, the environments in which they typically occur, and the effects of cognitive fatigue on each error mode; it is based on social psychology research conducted by Searle (1980) and Mandler (1975).
According to this literature, mistakes, slips and lapses cause accidents because they result in a worker’s failure to perceive that an event has occurred (e.g., that a bulldozer has begun to mobilize); failure to diagnose the nature of an event and to determine the necessary remedial actions (e.g., failure to recognize the need to change physical location when a bulldozer’s track has broken); and failure to implement those responses in a timely manner. In all cases, mental fatigue increases the potential for human error in occupational environments.
Table 2. Human Error, Work Environment & Impacts
| Human error | Definition | Susceptible environments | Impact of cognitive fatigue |
| Mistakes | Intentional planning related error (e.g.,) skill-based errors) | Dynamic work environments are prevalent and standardized work processes do not ensure sufficient worker-hazard interactions | Mistakes become more common as workers' judgment deteriorates during extended periods of work and mistakes remain undetected due to supervisor fatigue. |
| Slips | Unintended erroneous actions that result from mental distractions in familiar work environments | Typical work environments with one or more unusual external distractions | Distractions have a greater effect as workers have increasing difficulty focusing on their work tasks |
| lapses | Unintended erroneous actions that result from temporary memory failure | Typical work environments | Memory Failures increase dramatically during periods of mental fatigue |
Impact of Fatigue on Quality of Life
While no studies directly associate cognitive or localized muscular fatigue to quality of life, a well established body of literature links the whole body (i.e., general fatigue) to several ill personal effects. As noted, little is known about the immediate effects of fatigue on task achievement, work quality or teamwork.
| Human error occurs in a limited number of forms. These include intentional erroneous actions (mistakes and violations) and unintentional erroneous actions (slips and lapses). The fundamental difference between these is that mistakes are planning errors while slips and lapses are the result of failures in execution. |
Conversely, a relatively wide body of knowledge is related to the long-term effects of fatigue on workers (i.e., quality of life effects). Sparks, Cooper, Fried, et al. (1997), and van der Hulst (2003) reviewed most studies on long work hours and concluded that such hours can negatively influence health and well-being. Most significantly, overtime work leads to prolonged insufficient recovery that is assumed to disturb physiological processes and, as a consequence, induce health problems (Geurts & Sonnentag, 2006). Andersen (1970) showed that if one did not stop at registered sicknesses but also considered gastrointestinal irregularities and other health defects of limited direct medical significance, one would find negative effects of shift work on health.
Fatigue has been shown to cause significant and frequent health impacts such as coronary disease, hypertension (Dembe, Erickson, Delbos, et al., 2005), diabetes (Harma, 2006), insomnia (Taris, Beckers, Dahlgren, et al., 2007) and injuries (Sparks, et al., 1997) among workers in multiple industries.
Additionally, fatigue that results from extended work periods has been linked to adverse behavior and habits such as an unhealthy diet, lack of exercise and smoking,which, in turn,may cause health problems (van der Hulst, 2003).
Several Japanese studies found that extremely long working hours (systematically working more than 60 hours a week) can have severe effects on health, such as karoshi (death from overwork) and karojisatsu (suicide due to overwork) (Amagasa, Nakayama & Takahashi, 2005; Kawakami & Haratani, 1999; Nishiyama & Johnson, 1997; Sokejima & Kagamimori, 1998; Uehata, 1991). Lagging indicators of fatigue are summarized in Table 3.
Table 3. Lagging Indicators of Fatigue.
| Effects of fatigue on performance | Quality of life impacts |
| Reduction in quality | Gastrointestinal irregularities |
| Reduction in productivity | Coronary heart disease |
| Increased severity of injuries | Stress |
| Increased frequency of injuries | Hypertension |
| Sleep complaints | |
| Injuries at home | |
| Slow recovery from illness | |
| Unhealthy diet | |
| Lack of exercise | |
| Smoking | |
| Suicide due to overwork | |
| Cardiovascular disease. |
Fatigue Mitigation Strategies
Based on causal factors and individual risk factors, some potential countermeasures for cognitive and localized muscular fatigue are obvious. They include allowing workers to control their overtime shifts; providing rewards for participating in overtime shifts; and precluding some workers based on age, preexisting conditions and circadian rhythms. Several studies have investigated specific countermeasures for fatigue in construction. Goldenhar, et al. (2003), created a list of countermeasures and controls for fatigue (Table 4).
| Fatigue has been shown to cause significant and frequent health impacts. Fatigue that results from extended work periods has been linked to adverse behavior and habits such as an unhealthy diet, lack of exercise and smoking, which, in turn, may cause health problems. |
Other studies have investigated job rotation as a control for both types of fatigue. According to Jonsson (1998), job rotation is a method of rotating workers across various tasks that have different physical and mental demands over time and it is a promising method to manage worker fatigue. Job rotation has been implemented in many settings including refuse collecting (Neter, Wasserman & Kutner, 1990), cashiering and poultry processing (Henderson, 1992). Jonsson (1998) claimed that this strategy is ideal for construction because it is especially useful for dynamic tasks that require variations in muscular load. Furthermore, job rotation reduces errors and increases employee job satisfaction. Developing a proper job rotation plan involves determining which jobs to include, the rotation sequence and the proper rotation interval (Tharmaphornphilas & Norman, 2004).
A more advanced technique is to rotate workers based on a specific policy, such as choosing not to assign a worker to two stressful tasks in succession (Henderson, 1992). Carnahan, Redfern and Norman (2000) proposed a method to reduce low back injury in a manual lifting environment by implementing a genetic algorithm to provide multiple good job rotation schedules; they then used a clustering method to determine a general set of rules governing task exposure for each group of workers.
One must note several limitations of job rotation in construction. First, job rotation may not be realistic for some tasks that require a relatively high level of skill. Second, job rotation must be strategic as a poor rotation plan can increase risk for some workers. A poorly designed job rotation plan can actually increase worker stress.
Table 4. Preventive & Management Methods for Fatigue
| Preventative Measures | Countermeasures for fatigue |
| Control over overtime | Provide workers with more breaks-approximately 10 to 15 minuets every 2 hours |
| Rewards for overtime | Allow workers to rest and provide shade or air conditioning |
| Allow for schedule control | Have food and water available for workers and encourage them to remain satiated and hydrated |
| High work time control | Heighten supervision activities when workers are exposed to heat |
| Frequent alternation of shifts | Decrease pave in the heat and during extended work periods |
| 4-12-20 or 7-15-23 shifts | Take frequent rest breaks and encourage coworkers to do the same |
| Stabilize shifts | Self monitor physical and mental fatigue |
| Job rotation | Ask for help lifting heavy materials and note that strength diminishes with increased fatigue |
| Reduce frequency of successive high-stress activities | Work with a partner during extended work periods |
| Begin the workday earlier to reduce heat exposure during summer months | Increase teamwork |
| Limit the number of consecutive hours and days worked | Studies have investigated specific countermeasures for fatigue in construction. Goldenhar, et al. (2003), created a list of countermeasures and controls for fatigue. |
| "Over supervise" by reducing the ratio of workers to supervises | |
| Increase planning and frequency of safety meetings when workers are being pushed |
Fatigue Risk Management Model
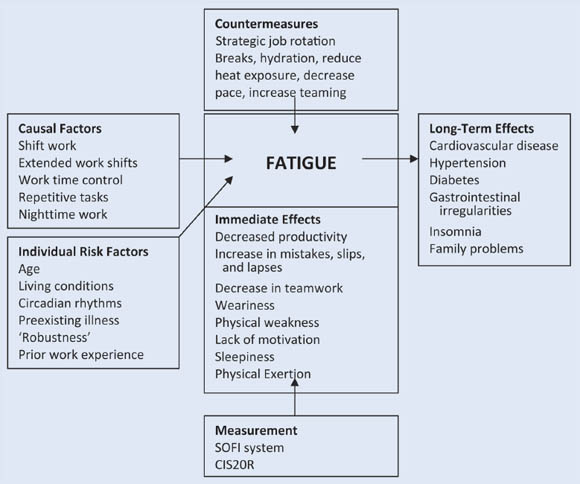
The body of literature reviewed was compiled to create a model (Figure 2) for fatigue risk management during rapid renewal highway construction projects. Particular attention is paid to leading and lagging factors and the immediate and long-term effects.
This model is intended to be used as a quick reference and summarizes the key points from the literature. It is expected that this model can be used by project managers and safety managers to identify, analyze and respond to fatigue risk factors. The discussions in this article and the numerous references provided can help readers gain a better understanding of fatigue causes, effects and countermeasures.
Conclusions & Recommendations
While numerous studies focus on occupational fatigue, no previous studies have attempted to summarize the literature in a cohesive document to mitigate risks in an emerging work environment. Furthermore, no studies specifically focus on the effects of rapid renewal scenarios or the potential effects of cognitive fatigue on human error.
| This model is intended to be used as a quick reference and summarizes the key points from the literature. It is expected that this model can be used by project managers and safety managers to identify, analyze and respond to fatigue risk factors. |
This article provides such a summary and addresses these key points. As this analysis reveals, construction worker fatigue may affect project success and workers’ quality of life. Specific controls and countermeasures have been developed in manufacturing, aviation, transportation and healthcare that may have direct application to construction.
The author suggests future research on several topics related to fatigue. First, the effects of construction- specific work tasks on fatigue should be evaluated through objective and rigorous research. Second, the impacts of fatigue on work performance (e.g., productivity and safety) should be measured and compared using activity sampling and safety metrics. Other types of fatigue, such as sleepiness and loss of motivation and concentration, should be highlighted. Finally, the efficacy of the controls noted in this article should be objectively studied.
This article is not intended to be all-inclusive. Rather, the objective was to discuss the various factors that may influence fatigue on rapid renewal highway projects; review the validated methods of measuring fatigue; and highlight how fatigue may influence work performance and quality of life.
Figure 2: Fatigue Management Model
References
Aanonsen, A. (1964). Shift work and health. Oslo, Norway: Universitetsforlaget.
Akerstedt, T. (1988). Sleepiness as a consequence of shift work. Sleep, 11(1), 17-34.
Ala-Mursula, L., Vahtera, J., Kivimaki, M., et al. (2002). Employee control over working times: Associations with subjective health and sickness absences. Journal of Epidemiology and Community Health, 56(4), 272-278.
Ala-Mursula, L., Vahtera, J., Kouvonen, A., et al. (2006). Long hours in paid and domestic work and subsequent sickness absence: Does control over daily working hours matter? Occupational and Environmental Medicine, 63(9), 608-616.
Ala-Mursula, L., Vahtera, J., Linna, A., et al. (2005). Employee work time control moderates the effects of job strain and effortreward imbalance on sickness absence: The 10-town study. Journal of Epidemiology and Community Health, 59(10), 851-857.
Ala-Mursula, L., Vahtera, J., Pentti, J., et al. (2004). Effect of employee work time control on health: A prospective cohort study. Occupational and Environmental Medicine, 61(3), 254-261.
Amagasa, T., Nakayama, T. & Takahashi, Y. (2005). Karojisatsu in Japan: Characteristics of 22 cases of work-related suicide. Journal of Occupational Health, 47(2), 157-164.
Andersen, J.E. (1970). Three-shift work. A socio-medical survey. Copenhagen: Teknisk Forlag.
Andlauer, P. (1960). The effect of shift-working on the worker’s health. OEEC Trade Union Information, 29, 3-9.
Ashburg, E., Gamberale, F. & Kjellberg, A. (1997). Perceived quality of fatigue during different occupational tasks: Development of a questionnaire. International Journal of Industrial Ergonomics, 20(2), 121-135.
Beckers, D., van der Linden, D., Smulders, P., et al. (2004). Working overtime hours: Relations with fatigue, work motivation and the quality of work. Journal of Occupational and Environmental Medicine, 46(12), 1282-1289.
Bills, A. (1934). General experimental psychology. New York: Longmans, Green and Co.
Bjerner, B., Holm, A. & Swensson, A. (1948). Om natt och skiftarbete. Statens Offentliga Utredningar, 51, 87-160.
Bruusgaard, A. (1969). Shift work as an occupational health problem. Studia Laboris et Salutis, 4, 9-14.
Bureau of Labor Statistics (BLS). (2007). Occupational injuries/illnesses and fatal injuries profiles. Washington, DC: U.S. Department of Labor, Author.
Carnahan, B.J., Redfern, M.S. & Norman, B.A. (2000). Designing safe job rotation schedules using optimization and heuristic search. Ergonomics, 43(4), 543-560.
Colquhoun, W.P. (1971). Circadian variations in mental efficiency. In W.P. Colquhoun (Ed.), Biological rhythms and human performance (pp. 39-107). New York: Academic Press.
Dembe, A., Erickson, J., Delbos, R., et al. (2005). The impact of overtime and long work hours on occupational injuries and illnesses: New evidence from the United States. Occupational and Environmental Medicine, 62(9), 588-597.
Fenwick, R. & Tausig, M. (2001). Scheduling stress: Family and health outcomes of shift work and schedule control. American Behavioral Scientist, 44(7), 1179-1198.
Folkard, S. & Akerstedt, T. (2004). Trends in the risk of accidents and injuries and their implications for models of fatigue and performance. Aviation, Space and Environmental Medicine, 75,A161-A167.
Geurts, S. & Sonnentag, S. (2006). Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scandinavian Journal of Work, Environment and Health, 32(6), 482-492.
Geurts, S., Taris, T., Kompier, M., et al. (2005). Work-home interaction from a work psychological perspective: Development and validation of a new questionnaire, the SWING. Work and Stress, 19(4), 319-339.
Gillberg, M., Kecklund, G. & Akerstedt, T. (1994). Relations between performance and subjective ratings of sleepiness during a night awake. Sleep, 17(3), 236-241.
Goldenhar, L., Hecker, S., Moir, S., et al. (2003). The “Goldilocks model” of overtime in construction: Not too much, not too little, but just right. Journal of Safety Research, 34(2), 215-226.
Hakkinen, S. (1969). Adaptability to shift work. Studia Laboris et Salutis, 4, 68-80.
Harma, M. (2006). Workhours in relation to work stress, recovery and health. Scandinavian Journal of Work, Environment and Health, 32(6), 502-514.
Henderson, C.J. (1992). Ergonomic job rotation in poultry processing. Advances in Industrial Ergonomics and Safety, 4, 443-450.
Hinze, J. (2006). Construction safety. Upper Saddle River, NJ: Prentice Hall.
Jacobs, J. & Gerson, K. (2004). The time divide: Work, family and gender inequality. Cambridge, MA: Harvard University Press.
Jansen, N., van Amelsvoort, L., Kristensen, T., et al. (2003). Work schedules and fatigue: A prospective cohort study. Occupational and Environmental Medicine, 60(1), 147-153.
Jonsson, H. (1998). Ernst Westerlund: A Swedish doctor of occupation. Occupational Therapy International, 5, 155-171.
Kashiwagi, S. (1969). Psychological rating of human fatigue. In K. Hashimoto, K. Kogi & E. Grandjean (Eds.), Methodology in human fatigue assessment (pp. 17-21). Kyoto: Taylor & Francis.
Kawakami, N. & Haratani, T. (1999). Epidemiology of job stress and health in Japan: Review of current evidence and future direction. Industrial Health, 37(2), 174-186.
Kinsman, R. & Weiser, P. (1976). Subjective symptomatology during work and fatigue. In E. Simonson & P. Weiser (Eds.), Psychological aspects and physiological correlates of work and fatigue (pp. 336-405). Springfield, MA: CC Thomas.
Lewis, G. & Wessely, S. (1992). The epidemiology of fatigue: More questions than answers. Journal of Epidemiology and Community Health, 46(2), 92-97.
Leung, A., Chan, C., Ng, J., et al. (2006). Factors contributing to officers’ fatigue in high-speed maritime craft operations. Applied Ergonomics, 37(5), 565-576.
Mandler, G. (1975). Mind and emotion. New York: Wiley.
Matthews, G. & Desmond, P. (1998). Personality and multiple dimensions of task-induced fatigue: A study of simulated driving. Personality and Individual Differences, 25(3), 443-458.
McGirr, P. (1966). Health considerations: Shift work and health. Proceedings of the Production Engineering Research Association.
Menzel, W. (1962). Menschliche tag-nacht-rhythmik und schichtarbeit. Basel/Stuttgart, Germany: Schwabe.
Mott, P.E., Mann, F.C., McLoughlin, Q., et al. (1965). Shift work: The social, psychological and physical consequences. Ann Arbor, MI: University of Michigan Press.
Neter, J., Wasserman, W. & Kutner, M.H. (1990). Applied linear statistical models (3rd ed.). Irwin, IL: McGraw-Hill/Irwin.
NIOSH. (2001). Building safer highway work zones: Measures to prevent worker injuries from vehicles and equipment [NIOSH Publication No. 2001-128]. Cincinnati, OH: U.S. Department of Health and Human Services, CDC, Author.
Nishiyama, K. & Johnson, J. (1997). Karoshi: Occupational health consequences of Japanese production management. International Journal of Health Services, 27(4), 625-641.
Oginski, A. (1966). Comparative research into the work on three shifts: Morning, afternoon and night. Proceedings of the 15th International Congress on Occupational Health, Vienna (pp. 384-385).
Okogbaa, O.G., Shell, R.L. & Filipusic, D. (1994). On the investigation of the neurophysiological correlates of knowledge worker mental fatigue using the EEG signal. Applied Ergonomics, 25(6), 355-365.
Ostberg, O. (1973). Circadian rhythms of food intake and oral temperature in morning and evening groups of individuals. Ergonomics, 16(22), 203-209.
Patkai, P. (1971). The diurnal rhythm of adrenal secretion in subjects with different working habits. Acta Physiologica Scandinavica, 81(1), 30-34.
Piper, B. (1989). Fatigue: Current bases for practice. In S. Funk, E. Tomquist, M. Champagne, et al. (Eds.), Key aspects of comfort (pp. 187-189). New York: Springer.
Rasmussen, J., Pejtersen, A. & Goldstein, L. (1994). Cognitive systems engineering. New York: John Wiley and Sons.
Reason, J. (1990). Human error. New York: Cambridge University Press.
Saito, Y. & Kashiwagi, S. (1970). Factors underlying subjective feelings of fatigue. Journal of Science Labour, 46, 205-224.
Sauer, J., Wastell, D.G., Hockey, G., et al. (2002). Effects of display design on performance in a simulated ship navigation environment. Ergonomics, 45(5), 329-347.
Searle, J.R. (1980). The intentionality of intention and action. Cognitive Science, 4 47-70.
Siegrist, J. (1996). Adverse health effects of high effort-low reward conditions at work. Journal of Occupational Health Psychology, 1(1), 27-43.
Siegrist, J. (1998). Adverse health effects of effort-reward imbalance at work. In C.L. Cooper (Ed.), Theories of organizational stress (pp. 190-204). New York: Oxford University Press.
Sokejima, S. & Kagamimori, S. (1998). Working hours as a risk factor for acute myocardial infarction in Japan: A case-control study. BMJ, 317, 775-780.
Sparks, K., Cooper, C., Fried, Y., et al. (1997). The effects of hours of work on health: Ameta-analytic review. Journal of Occupational and Organizational Psychology, 70, 391-408.
Taris, T., Beckers, D., Dahlgren, A., et al. (2007). Overtime work and well-being: Prevalence, conceptualization and effects of working overtime. In S. McIntyre & J. Houdmont (Eds.), Occupational health psychology: European perspectives on research, education and practice (Vol. 2). Maia, Portugal: ISMAI.
Tharmaphornphilas, W. & Norman, B. (2004). A quantitative method for determining proper job rotation intervals. Annals of Operations Research, 128(1-4), 251-266.
Thüs-Evensen, E. (1958). Shift work and health. Industrial Medicine, 27, 493-497.
Transportation Research Board. (2009). Implementing the results of the second strategic highway research program: Saving lives, reducing congestion, and improving quality of life. Washington, DC: National Academies Press.
Tucker, P. & Rutherford, C. (2005). Moderator of the relationship between long work hours and health. Journal of Occupational Health Psychology, 10(4), 465-476.
Uehata, T. (1991). Long work hours and occupational stressrelated cardiovascular attacks among middle-aged workers in Japan. Journal of Human Ergology, 20(2), 147-153.
van der Hulst,M. (2003). Long work hours and health. Scandinavian Journal ofWork, Environment and Health, 29(3), 171-188.
Walker, J. (1966). Frequent alternation of shifts on continuous work. Occupational Psychology, 40, 215-225.
Wild, H.W. & Theis, H. (1967). Der einfluss des schichtbeginns auf die unfallhaufigkeit. Gluckauf, 103, 833-838.
Wilkinson, R. (1971). Hours of work and the 24-hour cycle of rest and activity. In P.B. Warr (Ed.), Psychology at work (pp. 31-54). London: Penguin Books.